Outbreak Investigations: Analysing and Communicating Outbreak and Control Measures
Describing the outbreak is half the battle. Now that you understand how data can help you assess what caused the outbreak, the outbreak management team (OMT) will need to analyse the information gathered when describing an outbreak to ensure appropriate infection control measures are implemented. In this module you will learn how to analyse the information/data gathered about the outbreak, define a hypothesis that accurately describes the potential cause of the outbreak, identify and implement the appropriate control measures, and communicate outbreak findings. These activities will help end the outbreak and prevent reoccurrence.
Learning Objectives
By the end of this module you will be able to:
- develop an accurate hypothesis to describe a health care-associated infection (HAI) outbreak;
- explain how to test and redefine the hypothesis as new information is discovered;
- identify control measures that will aid in ending the outbreak and preventing reoccurrence; and
- develop a communication plan that informs public health officials and health care workers (HCWs) of the measures that have been put in place.
Learning Activities Estimated time:
-
Analyse the Outbreak (5 min)
In the previous module, you learned how to effectively describe an outbreak when it occurs. The first 5 steps of an outbreak investigation describe the outbreak.
In this module, you will learn about the next 5 steps of an outbreak investigation, including outbreak analysis and hypothesis development, control measures implementation, and communications.
- Develop hypotheses
- Evaluate hypotheses
- Refine and re-evaluate the hypothesis (if necessary)
- Implement control and prevention measures
- Communicate findings
Before we move on, let us recap describing the outbreak. Use the drop-down menu below to match the steps of the first part of an outbreak investigation with the examples from the neonatal intensive care unit (NICU) case study:
Now we are ready to move on with analysing the outbreak. Let us take a look at our case study for some more information.
Our OMT has looked through previous surveillance data. Between July and September 2 MRSA cases were isolated. Between that time and the fourth quarter (October—December) 5 cases were reported. Cultures sent to the lab from July to September returned 1.8% positive (107 cultures sent). Cultures sent to the lab between October and December returned 4.7% positive (106 cultures sent).
After receiving notification of results for patient 2, nursery staff began implementing control measures including ensuring:
- transmission-based precautions and isolation were in place for colonized/infected neonates;
- strict adherence to hand hygiene (alcohol-based handrub [ABHR] or soap and water); and
- measures for traffic control in the nursery, operation theatre, and labour room were put in place by locking doors so no one could enter without permission.
After another MRSA case was identified, additional control measures were implemented by infection prevention and control (IPC) professionals and the OMT:
- protocols for terminal cleaning of all patient care areas were re-emphasized and extensive training for housekeeping staff was provided;
- protocols for patient and staff screening, as well as environmental culturing, were put in place;
- new admissions to the NICU were suspended until currently admitted neonates were discharged and measures were put in place to avoid overcrowding;
- ABHR sanitizers were placed between each incubator; and
- a fixed schedule was implemented for visitors.
As we move through the following learning activities, keep this example in mind. Imagine how the OMT would approach each of the following steps.
-
Step 6 Developing a Hypothesis (5 min)
As you learned in the previous module, the descriptive and analytic processes often overlap. Many of the steps to develop a hypothesis take place during the initial steps of the outbreak investigation.
A hypothesis is a statement that predicts a relationship between two variables. This tentative statement proposes a possible explanation for a phenomenon or event. In an outbreak, the hypothesis poses an estimate as to what the source of the outbreak is. This estimation is based on the results of an initial investigation of the patterns seen in person, time, and place; the epidemiological links drawn from the descriptive data; and the patterns seen in clinical and laboratory results. The hypothesis must address the possible source, mode of transmission and exposure that resulted in disease. Based on the information you gathered, you will develop a hypothesis as to why and/or how the outbreak occurred.
An element, feature or factor that is liable to vary or change.Steps to Developing the Hypothesis
- Review the available data (line list, map and/or epidemic curve).
- Look for the patterns that emerge from the data or outliers.
- Review the information available in the literature and talk to experts (e.g., public health, infectious disease physicians, hospital epidemiologists, statisticians).
- Meet with affected patients to discuss their symptoms and exposures (if necessary).
- Administer a questionnaire to gather details of their exposure.
-
Steps 7 & 8 Testing the Hypothesis (5 min)
Once the OMT has decided on a hypothesis that describes the probable source of the outbreak, it is time to test the hypothesis. This is done by carrying out analytical studies and looking for and comparing patterns. Consider analysing patterns in:
- clinical data
- laboratory data
- epidemiologic data
- environmental studies
- staffing records.
Look for risk factors with significant differences between patients with the outbreak infection compared to patients without the infection. There are epidemiological/statistical methodologies that can be conducted to test the hypothesis. However, some challenges may impact the ability to test a hypothesis. These may include:
- low number of cases
- specimen collection no longer possible or insufficient
- lack of laboratory capacity
- negative publicity for the facility
- reluctance of patients to participate.
Testing the Hypothesis at the Neonatal Unit
Laboratory data was reviewed. Although molecular typing was not available, it was noticed that antibiotic susceptibility patterns for all five neonates were the same. Subsequent screening cultures from other admitted neonates were negative. Environmental cultures were also found to be negative. All staff in the nursery were screened for MRSA through collection of specimens from their nostrils, hands and hairline.
MRSA was detected in nasal cultures from one nurse while the remaining staff cultures were found negative. The susceptibility pattern for MRSA isolated from the nurse was similar to the susceptibility pattern for outbreak isolates derived from the clinical samples of the neonates.
The positive HCW underwent decolonization therapy consisting of five days of mupirocin nasal ointment twice a day and a daily chlorhexidine bath. The HCW was moved to a low-risk area (outpatient clinic) during this time frame. Screening was repeated 10 days after completing the decolonization therapy and the HCW was found to be negative for MRSA. The HCW returned to regular duties and there were no further cases.
Infected neonates were treated with vancomycin according to laboratory susceptibility reports and discharged. All were healthy on follow-up visits.
-
Step 9 Implementing Infection Control Measures (10 min)
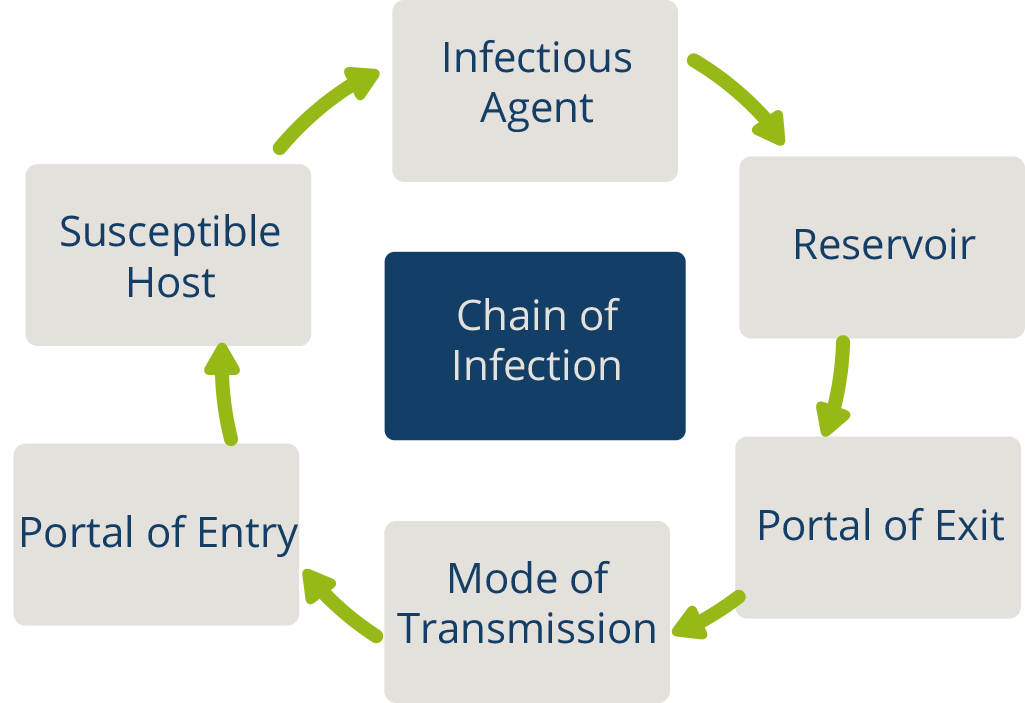
After you have analysed and tested your hypothesis, you can establish or re-establish appropriate IPC measures to interrupt transmission during outbreaks. As mentioned before, the steps of an outbreak investigation do not happen in a linear fashion. In the previous part, you learned that IPC control measures can be implemented at the start of an outbreak investigation in order to stop or slow the spread of disease. Recall the chain of infection. Breaking that chain is accomplished through the implementation of infection control measures that target specific approaches and may be divided into three phases:
- Short term: Immediate, specific measures needed to stop the outbreak (eliminate, isolate or quarantine the source).
- Medium term: Measures to prevent a future outbreak (transmission-based precautions, hand hygiene, etc.).
- Long term: Measures to ensure and maintain a culture of safety (immunizations, antibiotics, education).
An important approach of the infection control processes is to put in place measures to prevent a recurrence over the medium and long term. This is a quality improvement strategy and addresses the root cause of what went wrong. It keeps asking the question “why?”, even after immediate control interventions have been put in place. The infection control focal person, in consultation with the OMT, must continually assess the control measures and identify those that will require additional resources to prevent future outbreaks and promote a culture of safety.
Although most outbreak response and control measures involve source control and breaking transmission, the best approach to implement the intervention is using a multimodal strategy. The list below explains how to implement the 5 elements of a multimodal strategy in this context:
- the right practices, i.e., standard precautions at all times and implementation of appropriate transmission-based precautions depending on the mode of transmission (teach it): training HCWs on policies and procedures;
- environmental and engineering controls (build it): supplying ABHR and personal protective equipment (PPE), assigning additional personnel to outbreak areas, etc.;
- administrative controls (live it): leadership from senior administration pledging their support in stopping the outbreak;
- monitoring and feedback (check it): ensuring outbreak recommendations are being followed routinely and using laboratory surveillance to detect new cases; and
- reminders/communications (sell it): holding daily outbreak meetings, updating frontline staff, etc.
To prevent the transmission of infection within a hospital, one of the links in the chain of infection must be "broken". Of the six links which make up the chain of infection, we have the least control over the agent, the source and the host. On the other hand, we do have a great deal of control over the mode of transmission, the weakest link in the chain and the easiest to break. By implementing measures that interrupt transmission, we can prevent pathogenic microorganisms from reaching or entering a susceptible host.
When an outbreak occurs, it often exposes gaps in current infection prevention practices and measures. Corrective measures that are put in place can be temporary until the outbreak is resolved (e.g., bathing all patients with chlorhexidine to reduce microbial counts on the skin), or in other cases, may be measures that will be in place for the long term (e.g., a communication tool or sign to indicate a suspect or confirmed case requiring enhanced cleaning and/or PPE).
Unlike general IPC strategies instituted at the onset of an outbreak, more targeted or specific measures are based on findings of the investigation and evolve as new information is obtained. These measures should be implemented based on the type of pathogen involved (taking into account modes of transmission, reservoirs etc.) and the characteristics of the population at risk. Measures may include:
- elimination of contaminated products or equipment
- correction of clinical techniques or procedures
- modification of nursing procedures and processes
- identification and treatment of carriers (i.e., MRSA decolonization).
The infection prevention measures should be evaluated periodically for efficacy and, in some cases, to assess whether they are still needed (e.g., universal screening [screening of all patients admitted to a health facility] regardless of risk factors for a particular antimicrobial resistant organism or multidrug-resistant organism).
Now let us delve a little deeper into three additional categories of interventions for infection control measures. Click or tap the tabs below to read more about these interventions.
Control the Source of the Infection
Measures to remove the source of infection may include:
- excluding colonized HCW(s) from work
- shutting down contaminated water source
- discarding contaminated IV fluids
- strengthening disinfection and sterilization
- closing down the ward and limiting admissions to critical admissions only
- eliminating contaminated equipment and devices.
To apply some of these measures, it is important to identify the source of infection through patient and health personnel screening and surveillance. Examples include:
- screening of patients before admission into intensive care units
- screening kitchen staff for salmonella infection
- screening patients with new or worsening cough for tuberculosis.
Interrupt Transmission Routes
These measures will interrupt the various routes of transmission:
- Ensure compliance with standard precautions at all times.
- Monitor and ensure hand hygiene at the right moments according to WHO 5 Moments, check whether hand hygiene (including ABHR) supplies are available at the point of care and ensure hand hygiene is performed using the correct technique.
- Ensure that PPE is available, adequate, and is in fact used when indicated.
- Institute contact, droplet or airborne precautions according to risk assessment and mode of transmission
- Ensure care practices are modified in accordance with best practices and the safety of both staff and patients.
- Reduce HCW workloads.
- Strengthen environmental cleaning and disinfection. You may want to increase this activity during times of HAI outbreaks to ensure the environment remains low in microbial contamination.
- Ensure that decontamination and sterilization of reusable devices and equipment is performed according to best procedures and quality gold standards.
Hand hygiene is a fundamental IPC principle and is a key element in managing a HAI outbreak by breaking infection transmission. A key element during an outbreak is to observe staff performing hand hygiene to identify lapses or breaches according to the WHO 5 Moments of Hand Hygiene. Take the Standard Precautions Hand Hygiene module to learn more.
Protect the Population at Risk
This is often the least used intervention in the hospital setting. In most hospital outbreaks, there is no vaccine for commonly involved agents, many of which are organisms of human flora. Protecting vulnerable patients and staff is achieved by monitoring, developing a hypothesis about the potential source of the outbreak, identifying cases and risk factors, and implementing appropriate protective measures. Specific examples of interventions for protecting the population include:
- vaccination (if available or relevant to the outbreak at hand)
- environmental cleaning and disinfection
- equipment sterility.
One example of protection often used in hospitals is the use of chemoprophylaxis, for example, staff or contacts may be offered ciprofloxacin in the event of a meningitis outbreak or the use of antivirals (Tamiflu) for an influenza outbreak for patients and staff who are not immunized.
In the NICU case example, consider short-, medium- and long-term interventions to stop and prevent future outbreaks. Answer the questions below to identify interventions for this case.
-
Knowledge Check (5 min)
-
A Multimodal Approach to Outbreak Prevention (10 min)
As you learned in the previous activity, some control measures call for a multimodal approach. This is to ensure that measures to prevent reoccurrence of an outbreak are implemented systematically. Having a robust IPC programme is key to preventing and controlling an outbreak. Even if an outbreak does occur, considering systemic factors will help identify gaps and develop action plans to target the areas of concern.
Implementing IPC practices is rooted in behaviour change. A multimodal approach is designed to achieve this. The following are principles that must be incorporated in a multimodal strategy:
- Build it focuses on infrastructure (e.g., access to running water, availability of supplies such as ABHR and soap).
- Teach it focuses on HCW training.
- Check it focuses on monitoring and feedback.
- Sell it focuses on advocacy, communication, and the use of prompts or reminders.
- Live it focuses on the organizational culture of safety.
In the example of the outbreak at the NICU, there were several IPC measures put in place. One measure was implementation of strict hand hygiene protocols with ABHR dispensers added throughout the nursery, including one between each incubator. Using the text boxes below describe how you would approach each principle of the multimodal strategy to address this activity.
Core Components
Part of a long-term strategy to provide clean, high-quality care within a climate of safety is to strengthen or create an IPC programme in your facility. When fully implemented, this approach should minimize the occurrence of HAI outbreaks. The WHO guidelines on core components of IPC programmes cover eight areas of IPC and provide 14 recommendations and best practice statements. They describe the evidence-based core elements of an IPC programme. To learn more about how putting these components in place can prevent an outbreak, take the Core Components and Multimodal Strategies module.
-
Step 10 Communication (5 min)
Now we can discuss the final step in outbreak investigation and management: communication. Good communication skills and strategy are essential to outbreak management and must be carefully planned. If you have a communications team or other such resources, be sure to notify them as soon as possible.
During the outbreak, the OMT should develop a strategy to regularly provide updates to and communicate with the following people:
- the head and staff of affected units within the hospital
- hospital administration and management
- patients and HCWs
- the public, if applicable
- the media, if applicable.
Communication is also important after the outbreak. A well-planned briefing should be provided to the hospital administration, affected units and other hospital staff, as well as the public health authorities of the government. Think of the steps of the outbreak investigation and what should be communicated from each stage of the investigation.
- Describe the source of the outbreak.
- Use epidemiological data to support the description.
- Detail the actions taken to control the outbreak.
- Describe steps taken to prevent and stop transmission.
- Construct a unified message to disseminate to media outlets.
- Consider community engagement strategies.
Communication efforts do not always include providing updates to external media. Media often become involved where there are unfortunate outcomes such as death or major disability, e.g., blindness or significant morbidity. When thinking about how you will communicate, keep in mind that communication involves a wide range of methods. Simply sending an email out to staff is not sufficient communication. In some situations, it may be more appropriate to meet in person to discuss the outbreak. You should also consider the limited availability of technology and the sensitive nature of some information that may need to be conveyed and be aware of any cultural sensitivities.
-
When the Outbreak Is Over (5 min)
After you have taken steps to properly communicate about the outbreak and interventions that have been implemented, you should think about what factors must be in place to consider the outbreak to be over. There are several points to think about with the OMT in deciding to declare that the outbreak is over:
- Has auditing and feedback been implemented, and do the results demonstrate compliance with IPC measures?
- Review the epi curve and incubation period: are cases declining?
- Depending upon the organism, in some instances an outbreak can be declared over when no new infections occur for a period equal to two incubation periods.
- Were the IPC measures and changes to practices able to be sustained?
- Have local public health partners been consulted? Their data should also be taken into consideration.
Continue to monitor and collect data until these factors indicate that the outbreak is showing signs of decline.
Outbreak Reporting
As the outbreak draws to a close, the IPC focal person/team should create a detailed report describing the outbreak, the investigation process, control measures and communication strategies. Use the 10 investigation steps to guide the development of the report.
The purpose of the report is to document the investigation and management of the outbreak, and to provide an opportunity for leadership to review this information and the events that unfolded. It also allows an opportunity for evaluation of and reflection on the process.
Often, once the outbreak is declared over, the team wants to get back to “business as usual”. However, it is important to set up a final debrief meeting to ensure that all parties involved understand how the HAI outbreak occurred in the first place, and why the interventions that the OMT has put in place worked to end it. This is an opportunity to review the report, discuss the outbreak and focus on some key questions. When having this debrief meeting, frame the conversation in terms of:
- what went well
- what the challenges were
- what needs to change for the future.
Preventing a similar outbreak and sustaining achieved improvements should be the outcome of this meeting. Be sure to identify which measures are medium or long term and the support and/or resources needed.
MRSA Outbreak Conclusion
A number of IPC-related measures were implemented, such as improved hand hygiene (including increased availability of products), improved environmental cleaning with extensive training of cleaning staff, changes to traffic flow within the unit and compliance with the flow, control of visitors, and decolonization of colonized HCWs and redeployment from the NICU to the outpatient department. The outbreak was declared over after no further MRSA cases were identified. Identification of an outbreak situation is essential for its control, and it often requires multiple IPC measures taken simultaneously to curb the outbreak.
Only a probable epidemiological link between the outbreak and the colonized HCW could be established. Typing of MRSA strains could not be performed and thus a molecular link was not ascertained and a true source for the outbreak could not be confirmed. While it is important that infection control measures be taken consistently at all times, these measures must be re‐emphasized when an outbreak occurs. Again, success is only truly achieved by way of a multimodal improvement strategy.
-
Knowledge Check (5 min)
-
Summary (5 min)
In this part, you have learnt how to investigate an outbreak by analysing it, implementing control measures and communicating effectively. Use the data collected to begin to explain the outbreak and address how the facility should react to it.
In the analysis phase, the OMT develops a hypothesis that accurately describes the HAI outbreak. The components of this hypothesis include the possible source, mode of transmission and exposure that resulted in disease. In order to demonstrate accuracy, a hypothesis must be tested. Often a hypothesis may need to be redefined as new information is discovered. Once the OMT has identified the source and modes of transmission, they can now pursue ways in which to break the chain of infection. Short-term measures are immediate and needed as soon as possible to stop the outbreak. Medium-term measures prevent a future outbreak. Long-term measures ensure and maintain a culture of safety. Using these methods to interrupt transmission will begin to control the outbreak. The OMT will adjust the control measures based on ongoing monitoring and analysis of the outbreak. As we know, this step of the investigation can occur alongside Step 1, at the start of the outbreak.
Communication during an outbreak is very important. You will need to identify who to maintain contact with to implement control methods and update the public on the status of the outbreak. Be sure the right people are notified. It is equally important to brief the public, nearby hospitals and other health facilities after the outbreak. Lastly, the OMT will need to report on the investigation in order to document the investigation and management of the outbreak, and to provide an opportunity for leadership to review this information and the events that unfolded.