Session 3: Fundamentals of HIV Testing Services
Counsellor Self Awareness
In this section, we will look at some of the psychological and social impacts of HIV. We will discuss the integrated framework for HIV counselling, and then consider our own values and how that plays a role in providing care and treatment. We will then discuss stigma and discrimination and how we can face our own biases, as well as list some strategies for dealing with stigma and discrimination in families and communities.
Learning Objectives
By the end of this session, you will be able to:
- Describe the integrated framework for counselling in HIV prevention, care, and positive living.
- Explain the concept of self-awareness.
- Discuss the importance self-awareness in counselling within the context of HIV and AIDS.
- Explain the concepts of stigma and discrimination in relation to HIV/AIDS.
- Outline the factors contributing to stigma and discrimination in HIV and AIDS.
- State the effects of stigma and discrimination.
- Discuss strategies that can be used to deal with stigma and discrimination within families, communities and other contexts.
Learning Activities
-
The Psychological Impact of HIV (10 min)
Charles, a 28-year-old married man with one child, is employed as an accountant. He and his wife are HIV-positive but their 3-year-old daughter has tested negative for HIV. During a business trip he met two friends, one is not married and the other is divorced. They have been going out drinking and Charles sometimes spends the weekend away from home. He has recently stopped supporting his wife and child. The wife is informally employed and has threatened to move out with the child to go and stay with her parents. In this scenario, we are confronted with so many issues that it becomes challenging to address them and provide care for the clients. The realities of life for these clients can cause a great amount of distress and lead to bigger issues.
As health workers we will not be able to solve all the problems that are presented to us. And we may not always agree with client’s lifestyles and choices. In this session we will touch on some of these issues and consider strategies for addressing them.
“The psychosocial impact of the AIDS epidemic is very considerable, taking into account that AIDS destroys the closest bonds between people; bonds that are relied upon to provide emotional and economic security, love, care, meaning in life, a sense of continuity and identity.” Source
Elizabeth Jareg, Special Advisor, Redd Barna OsloALL persons in a community are affected by HIV and AIDS, whether they are actually infected with the virus or not. The impact of HIV and AIDS is both psychological and social. Psychosocial involves aspects of social and psychological behaviour. It relates to one's psychological development in, and interaction with, a social environment.
HIV and AIDS links with other social problems affecting individuals, families, and communities today, including family violence and abuse, economic problems/poverty, separation and divorce, infidelity, bereavement, alcohol and drug use, some cultural practices (such as wife inheritance), some religious practices (such as denouncing condom use), and child abuse (particularly sexual abuse). Clients face a great many challenges that may not be apparent when they come in for testing. As health workers, it is important for us to consider that these broader issues can affect services. We need to keep this in mind to provide the best care possible.
Tap each tab to see examples of psychological and social effects of HIV and AIDS on the individual, family and community.
Psychological effects
- Grief
- Anxiety
- Fear
- Denial
- Anger
- Desolation
- Constant worry
- Pessimism about the future
- Helplessness
- Suicidal preoccupation
- Bereavement
- Shame
Social effects
- Family disintegration
- Economic destitution
- Rejection due to stigma and discrimination
- Early sexual activity of girl children to support families
- Social isolation due to stigma
- Unpredictable behaviour patterns
- Young children caring for younger sibling and/or sick parents
- Helplessness
- Increasing number of street children
- Being ill-understood
-
Extreme Consequences of HIV and AIDS (5 min)
There are times when you may see or experience more extreme consequences of HIV and AIDS. You may see a breakdown of social norms and traditions which have represented security. In extreme circumstances, you also can see a gradual depletion of community resources, human and material, and a labour crisis as the productive age group is diminished. Finally, under extreme circumstances, a community may experience a high ratio of most dependent persons, young and old, with no support.
As mentioned at the beginning of this section, HIV and AIDS may destroy close family and community bonds. These bonds may be between husband and wife, boyfriend and girlfriend, parents and children, grandparents and their children, siblings whose parents have died of AIDS, siblings who have had a sibling die of AIDS, and others.
We should try to pay attention to the needs of affected families and communities that emerge in the wake of the psychosocial effects of HIV and AIDS, and the destruction of the persons’ close bonds. We may need to assist with providing referrals for basic needs (food, safe water, shelter, love and belonging, etc.). We should also consider the client’s needs for:
- Empathy
- Empowerment through acknowledgment of efforts, strengths, and coping
- Being listened to
- Information on HIV and AIDS awareness, prevention, and management
- Answers to questions
- Feelings to be acknowledged and normalised
- Help to cope with their losses (bereavement counselling)
- Help to cope with other associated practical issues such as care of orphans
-
Bonds in Our Lives (10 min)
1. Take a moment to think about the many close bonds in your life. This can be family members, other relatives, friends, co-workers, neighbors, church members, or anyone you consider close in any way.
- Write down your bonds in your workbook.
- Now imagine how HIV and AIDS could affect the bonds you have listed.
- Look at someone you have named on your list and imagine that bond being destroyed by HIV and AIDS, put a line through the name.
- Think about how that made you feel losing bonds. Write down that feeling.
Try to remember this feeling of pain or loss or sadness when you are working with clients who have experienced HIV and AIDS destroying their families and communities. Use this to empathize with those clients and connect with them to provide compassionate care.
-
Framework for Integrated Counselling (10 min)
Integrated counselling is an approach which uses traditional counselling methods to address the multiple needs of those infected with HIV. It mixes biological information and medical technology with an understanding of the psychological and social dynamics of humans. Integrated counselling employs the counsellor, as a skilled aid, to help patients face the substantial challenges posed by HIV.
Goals
Integrated counselling aims to address the multiple challenges faced by those infected with or affected by HIV and AIDS. No single person or agency can provide for all the needs of people infected with or affected by HIV and AIDS.
The main goals of integrated counselling are to link PMTCT, HTS, clinical care, OI/ART, TB, nutrition, STI, CHBC, and follow up support services to reduce fragmentation and separation of these programs. This linkage will facilitate a continuum of care for patients at facilities and will help clients face the challenges of HIV and AIDS in the community and at facilities.
There are a wide range of services and service models that exist within health facilities in Zimbabwe, so what is available at one facility may not be identical to what is available in another facility. The overall goal is for each health facility to find its own way to use available resources to provide as comprehensive a range of services for clients as possible, and to integrate these services to the extent that this is feasible.
Tap on each part of the graphic to learn more about integrated care.
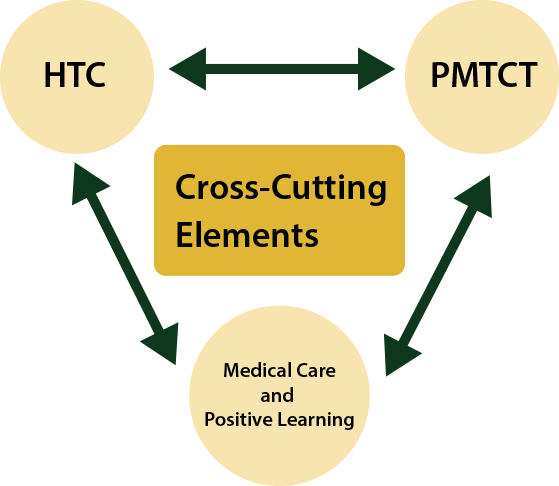
Cross-cutting Elements
- Disclosure and partner referral
- Prevention and risk reduction
- Social support for behavior change
- Planning for the future
- Answers to questions
- Adherence
PMTCT
- Uptake of services in pregnancy
- Infant feeding
Medical Care and Positive Learning
- Accessing medical care
- ARV, OI treatment
- Prevention
- Positive Living
HTC
- Behavior change
- Male circumcision
-
Loyce (15 min)
Watch the video about Loyce.
-
Stigma and Discrimination (5 min)
“Many people suffering from AIDS are not killed by the disease itself but are killed by the discrimination surrounding everybody who has HIV/AIDS.” Source
Nelson Mandela, 2002Tap on each term to learn more about it.
Stigma
Generally stigma implies the branding or labelling of a person or group of persons as being unworthy of inclusion in a human community, resulting in discrimination and ostracisation. The branding or labelling is usually related to some perceived physical, psychological or moral condition believed to render the individual unworthy of full inclusion in the community.
We may stigmatise those we regard as impure, unclean, or dangerous; those who are different from ourselves or live in different ways; or those who are simply strangers. In this process, we construct damaging stereotypes and perpetuate injustice and discrimination.
Stigma often involves a conscious or unconscious exercise of power over the vulnerable and “marginalised.” Source
A report on the Theological workshop focusing on HIV and AIDS related stigma. UNAIDS, February 2005, p.11We stigmatise when say things like:
- “She was promiscuous.”
- “He or she deserves it.”
- “He or she is risky.”
- “He or she is lame.”
- “He or she is not holy.”
Discrimination
Any distinction, exclusion, restriction or preference which is based on exclusionary perception or structures (e.g., race, belief, sexuality, gender, profession) which has a purpose or effects of nullifying or impairing the recognition, enjoyment or exercising by all persons, on equal footing of all rights and freedom. Discrimination is an action or treatment based on stigma and directed towards the stigmatised; it is sanctions, harassment, scapegoating and violence based on infection or association with HIV and AIDS.
Stigma is an attitude; discrimination is an act.
-
The Why and Where of Stigma and Discrimination (10 min)
There are many reasons that HIV and AIDS related stigma and discrimination occur. HIV and AIDS is a life-threatening disease, and people are scared of contracting HIV. Often the disease is associated with immoral behaviours (such as concurrent sexual partners, sex between men, or injecting oneself with drugs) that are already stigmatized in many societies. People have insufficient knowledge, myths, misconceptions, and fear about HIV transmission. We often see that PLHIV are thought of as being responsible for becoming infected. Other factors that contribute to the stigma and discrimination can be related to religious or moral beliefs that lead some people to believe that having HIV is the result of moral fault (such as promiscuity or 'deviant sex') that deserves to be punished.
In the early days of the HIV epidemic, a series of powerful, but sadly mistaken images were used that reinforced and legitimised stigmatisation. They portrayed the epidemic as a punishment (e.g., for immoral behaviour); as a crime (e.g., in relation to innocent and guilty victims); as a war (e.g., in relation to a virus which must be fought); and as a horror (e.g., in which infected people are demonised and feared).
Tap on each forms of HIV- and AIDS-related stigma and discrimination to read more.
Moral judgment
People are blamed for their ‘behaviour’. HIV is mostly a sexually transmitted disease, so people assume that the person has had many sexual partners.
Physical isolation
For example, people living with HIV or AIDS might be forced to eat alone. They may not receive any visitors or have physical contact with other people.
Separation
People not infected with HIV may see those who are infected as different (us versus them). This reaction is based on ignorance and fear of HIV and AIDS.
People treated as useless
People may be treated as though they can no longer make a contribution. This undermines self-esteem and self-confidence.
Stigma by association
Family members or orphans may be stigmatised; the family status and cohesion is affected.
Self-stigma
People living with HIV or AIDS blame themselves and isolate themselves from others.
Legislations
Compulsory screening and testing has caused limitations on international travel and migration. This has also affected people’s ability to become employed at some organizations or to qualify for life insurance.
Sectarianism
Compulsory screening may target risk groups based on lifestyle, skin colour, looks/appearance, and type of occupation.
Take a moment to think of examples of forms of discrimination that you are aware of. Type your answer in the box below, then tap the compare answer to compare your answer to an expert’s.
Causes of stigma and discrimiation
It is hard to pinpoint exactly what people’s motivations are for stigmatising and discriminating. Often it involves moralistic thinking and negative judgment–holding the view that HIV positive people are: sinners; promiscuous; unfaithful; ‘sleeping around sluts’. Some other causes could be people’s beliefs about modes of transmission, fear of infection, fear of the unknown, fear of death, ignorance–lack of knowledge and misconceptions which make people fear physical contact with PLWHIV.
We see stigma and discrimination show up in many different forms and places. Tap on each of the tabs below to read more about where stigma and discrimination may occur and what it can look like.
Workplace
- Workers shun and make comments about persons living with and suspected to have HIV.
- People living with HIV are viewed as unreliable and incapable.
- Bosses and/or superiors usually block any promotion or further studies and try to get rid of workers living with or they suspect to be infected with HIV.
School
- Children whose parents are living with HIV are treated badly.
- Rejection and name calling–they are at times made not to share seats and books with others, or made to eat alone in secluded corners.
- Teasing–basing on the information from their teachers or parents, some children adopt a teasing habit of their colleagues, such as:
- “Your father died because of immoral behaviour”
- “Your mother died because she was a prostitute”
- “You have a rash you cannot sit next to me, or swim with other children”
- “You are coughing, you have TB and HIV”
- Negative messages/slogans in schools (“AIDS kills. No sex before marriage.), suggests that all people with HIV have had sex.
- The result of stigma and discrimination in school is feeling isolated and/or depressed, concentration declines, which can lead to failure and dropping out from school.
Media
- Negative messages (“AIDS kills”). These promote fear and panic.
- They portray the image of PLHIV as those who are about to die, and have nothing to live for.
- Such negative messages are constantly repeated on radios, TVs or on billboards along the roads.
Faith groups
- Some self-righteous people presume that all people living with HIV have sinned or are promiscuous or adulterous or disobedient to God and are not morally upright.
- They mistakenly believe that such persons are being punished for not following God’s laws.
- Dilemma on how to manage Holy Communion especially sharing of utensils.
Effects of HIV and AIDS stigma and discrimination
When PLHIV are feeling stigma and discrimination, they may end up feeling fearful to disclose their HIV-positive status. This fear of disclosure often results in a lack of social support, lack of proper health care, further spread of infection (inability to change behaviour), increased psychosocial suffering, internalised shame, poor quality of life, and social isolation
Stigma and discrimination can leads to silence and denial – refusal to acknowledge and deal with HIV, and carry on with life. Because of ignorance and fear, resulting in allowing prejudice to thrive, risky behaviours go unchallenged and uncaring behaviour go unchanged. PLHIV remain silenced and side-lined (left out).
-
Responding to Stigma and Discrimination (5 min)
Before reading further, take just a moment to think about the following questions:
- What is my attitude towards people living with HIV and AIDS?
- Do I have any personal encounter with a person suffering from HIV and AIDS, and how do I feel about this person?
Most people infected with HIV are neglected by many in our communities due to fear of contracting HIV and the mistaken idea that it affects only those who are “different”, or out of the mainstream of the rest of society.
Questions for reflection: You don’t need to write down answers but just take a moment to consider your responses to the following questions:
- Have I ever helped someone to go for HIV testing?
- Have I helped people to gain accurate knowledge about the dangers of HIV and AIDS?
- Do I feel that those infected and affected by HIV and AIDS are just as important as I am?
- What have I done to help people living with, or, affected by HIV and AIDS?
People living with or affected with HIV and AIDS tend to lose hope and are living in fear for their future. Many people today deny that they have been or currently are at risk of contracting HIV, out of fear, pride, or ignorance. Others do not take advantage of HIV counselling and testing in order to learn their HIV status and thus be able to plan accordingly for their future lives.
As health workers it is important for us to accept those infected and affected by HIV and AIDS. That means that we should provide support of all kinds to those infected and affected by HIV and AIDS (emotional, spiritual, moral, material, etc.) according to our abilities and within our means.
We should also advocate for the rights and welfare of those infected and affected by HIV and AIDS within our families and communities emphasising fair treatment of PLHIV.
We owe it to ourselves and our clients to know the facts about HIV and AIDS so as to be able to deal with the myths and misconceptions that lead to stigma and discrimination.
-
Addressing Cultural Issues (5 min)
Culture andCulture is the habits, expectations, behaviours, rituals, values and beliefs that human groups develop over time. Culture is a product of the interaction of people, ideas and the physical environment. Through culture and tradition, people learn acceptable behaviour; what is right and wrong. Culture determines and influences social status. Culture determines and influences the use of language. Culture is dynamic.tradition and tradition influence how people interpret, explain, and respond to HIV infection and to AIDS. The appearance of a new or dangerous disease may prompt people to look for explanations of its origin. Sometimes they blame God or some other supernatural power. Sometimes they blame others for putting a curse on them or for using witchcraft. Sometimes patients blame themselves.An inherited, established, or customary pattern of thought, action, or behaviour (as a religious practice or a social custom) - Merriam Webster
Cultural beliefs about HIV and AIDS may affect how clients seek help and comply with treatment. The cultural beliefs of the client may play a role in how clients decide to return for follow-up sessions and if clients tell their family about needs related to the illness. For pregnant women, her cultural beliefs may be part of how she makes choices related to child-bearing, such as seeking out treatment for PMTCT, altering infant feeding practices, planning for orphan care if needed. Cultural beliefs may also affect how or if clients tell sexual partners about the need for HTS.
We must be sensitive to the way in which culture influences people’s response to HIV and AIDS. Different cultures have different rites and traditions for terminal illnesses, death and bereavement. Because HIV is transmitted sexually mainly, cultural and personal attitudes towards sex and sexuality are extremely important. Therefore, counsellors need to be sensitive to cultural differences, or admit unfamiliarity with the client’s culture if this is the case. Discuss cultural expectations about sex roles, sexuality, and childbearing, and anticipate that some information may be met with embarrassment, laughter, or anger depending on the cultural context.
-
Values Clarification (20 min)
Please complete the two self-assessment forms found in your workbook as honestly as possible. This exercise is intended to get you thinking about your own feelings about HIV and AIDS and how they relate to working with HIV-positive clients. This assessment is meant to be personal.
After completing the exercises consider the following:
- What surprised you most about your responses?
- How do your values affect your care of HIV-positive clients?
- How can you work to improve your care of HIV-positive clients given what you know and understand about your own values?
-
Defining Self-Awareness (5 min)
Self-examination and a clear understanding of one’s own values are essential to anyone working in the counselling field. One of the key qualities of an effective counsellor is a high degree of self-awareness. Self-awareness is your capacity to stand apart from yourself and examine your motives, history, scripts, actions, habits, and tendencies.
To be effective, you need to know how you function emotionally. If you are not in touch with yourself, your experiences, attitudes, and emotions, you cannot effectively help others. Just like the clients you see on a daily basis, you must face their own inner feelings about HIV and AIDS. Research and experience demonstrate the importance of providing counsellors-in-training with an opportunity to increase self-awareness.
By being self-aware, you are better able to communicate an attitude of equality, respect, and confidence. You can empathise without projecting your own feelings and needs onto the client in a way that will be detrimental to effective counselling. Part of your responsibility is to encourage clients to take responsibility for themselves.
Trigger issues
Counselling and health are fields that discuss issues human beings experience in their lives. Issues that clients disclose to HCW or counsellors may evoke emotions in the HCW or counsellor which may either hinder or help the counselling session. When the counsellor’s emotions erupt as a result of the issues a client raises in session, we say the counsellor has been triggered. Emotions may be triggered as a result of having experienced (or someone close having experienced) an issue personally. It is because of these triggers that you need
Think about how you responded to the values clarifications exercises. You might have identified some of your own triggers. Possible triggers include:
- Domestic violence
- Sexual abuse
- Orphan hood
- Infidelity
- Alcohol abuse
- Disability
- Separation and divorce
- Step-parenting
- Chronic illness (e.g., HIV and AIDS)
-
Developing Self-Awareness (10 min)
Although almost every HCW/counsellor has a family member or close friend who has died of AIDS, it’s usually not possible to discuss a relative’s illness openly with family members, or even with the person with AIDS, due to others’ collective denial. Most HCW/counsellors are unwilling to be tested for HIV themselves. They are also unwilling to discuss the risks of HIV within their own relationships.
Part of your responsibilities is to encourage clients to take responsibility for themselves. Thus, it is useful for you and your supervisors to assess your own needs and feelings continually and discuss them with peers and supervisors.
Tips for developing self-awareness
- Talk with others about your own life experiences, attitudes, and values
- Reflect upon your own feelings and reactions (introspection).
- Accept feedback—learn the effects of your behaviour from others.
- Participate in professional training or education.
- Debrief counselling sessions with other counsellors or a supervisor.
- Reflect on thoughts and feelings that come up during counselling sessions with clients.
- Know when to refer a client to a colleague if unable to handle.
JOHARI window
The JOHARI window is a concept developed by Joseph Luft and Harry Ingham (hence JOHARI). It is a tool used to develop understanding of the self through outlining what makes the self and what helps with self-discovery. It challenges our self-awareness, our ability to share ourselves with others, and our willingness to explore the unknown, and also offers a four-part presentation of ourselves. Tap each quadrant in the graphic below to learn more.
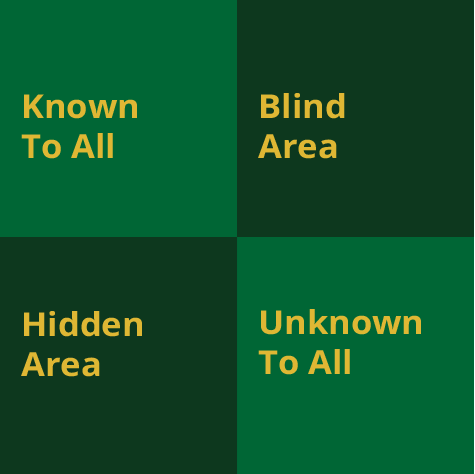
Known to All
This represents what we freely express for others to see, including our behavior and attitudes. The view can be extended by self-disclosure. This window refers to the aspects of oneself that you and other people know about you and are open to see. These aspects include such things as:
- Your physical outlook (i.e., height, complexion, weight and other physical features)
- Your gender (from the obvious)
- Your family (to those in your locality)
- Your educational level (to those in your locality)
Blind Area
We cannot see this area of ourselves; it is unknown to us, but others are aware of our behavior and body language. Our self-awareness can be extended by feedback from others. However the self may get to know about the blind self through feedback from the others as they share their opinions of you. You may agree or disagree with the feedback received and once you get to know about the feedback, it shifts from this window to window number one (the public self).
Aspects in this window may include the following:
- Your temper
- Your emotions
- Other perceptions that other people may have of you
Unknown to All
Closed to everyone. This represents parts of us both we and others are unaware of. Holds unconscious needs, impulses and anxieties, untapped potential. Counselling can bring these out to the open.
These constitute the unknown or undiscovered you, which may include such things as:
- What the future holds for you
- Your longevity
Hidden Area
This represents the private part of ourselves (e.g., our secrets, shame, guilt feelings, etc.). We are aware of it and choose not to share this part with others. Others may get to know about these aspects of yourself only if you decide to share these aspects of yourself with them
These issues may include:
- Your sexual orientation
- Your secrets
- Your past experiences
- Your dreams and fantasies
-
Key Points (5 min)
- Diagnosis with HIV disease and AIDS affects people physically, socially and emotionally.
- HIV infection can be a destroyer of close bonds.
- Integrated counselling aims to address the multiple challenges which are faced by those infected with HIV and AIDS.
- Illness, death and HIV and AIDS are looked at in different ways by different cultures and religions.
- Sigma is an attitcude, discrimination is a behavior.
- Stigma and discrimination negatively affects a person’s ability to get prevention, education, treatment, care and support.
- Self-awareness helps you to recognize your triggers and address potential impacts.
- We all must examine our personal values, beliefs and experiences to minimize influence on client services.