|
|
|
The Local Implications of a Bioterror Attack
Seattle-area hospitals, health departments, and emergency responders began conducting bioterror disaster drills several years before the 2001 attacks. During the World Trade Organization meetings in Seattle, bioterror surveillance took place.
Such readiness is critical. In the event of an intentional smallpox virus dispersal, for example, all Seattle hospitals, including those affiliated with UW Medicine, would be called upon to evaluate, treat, and quarantine potential cases. Basic preparation includes selecting appropriate health personnel for vaccination and ensuring that all clinicians understand the possible complications from smallpox vaccination.
“There’s an acute need for medical professionals and hospitals to be prepared for their role in both recognizing and responding to biological terrorism,” said Dr. Jeffrey Duchin, assistant professor of medicine and chief of the Communicable Disease Control, Epidemiology and Immunization Section of Public Health - Seattle & King County. “This is especially true for UW Medical Center and Harborview Medical Center, because of their leadership positions in the medical community for the whole WWAMI region.” The WWAMI region encompasses Washington, Wyoming, Alaska, Montana. and Idaho.
Public health authorities, hospitals, and clinicians are the immediate defensive line against bioterrorist attack. If the infective agent is identified quickly and accurately, widespread illness might be averted in some instances with antibiotics, vaccine, or antitoxin. Several commonly available antibiotics worked against the strain of anthrax released in autumn 2001. To assist in early identification, the UW’s School of Public Health and Community Medicine has provided bioterrorism preparedness training materials for primary-care clinicians.
|
|
|
 |
|
|
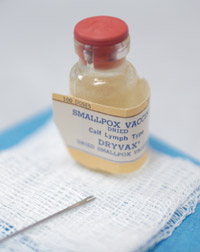
Vial of smallpox vaccine
|
|
|
|
|
The biggest concern is smallpox. The United States population is considered susceptible to this infectious disease. Many people have immune systems compromised by other illnesses, and would be more at risk for severe complications and fatalities. Additionally, the vaccine strain can spread from the person vaccinated to susceptible family members and other close contacts. Physicians will need to help patients understand their individual risks and benefits for vaccination.
In the 1970s, a containment strategy pioneered by UW medical alumnus Dr. William Foege eradicated smallpox from nature worldwide. His approach remains a key component of the planned first response: isolation of confirmed and suspected smallpox cases followed by tracing, vaccinating, and monitoring of the circle of contacts around each case.
This strategy might prove less effective today in the United States, where many people are highly mobile and immunological protection is so weak. In addition, bioterrorists could release the virus in several locations. In September 2002, to complement the ring vaccination strategy, the Centers for Disease Control adopted guidelines for mass vaccination of the U.S. population if there is evidence of more than limited spread. The plan envisages immunization of a million people over five to seven days and requires approximately 5,000 local public health workers to implement.
“Improving the capacity of health-care providers and hospitals to recognize and respond to any terrorist attack is a priority,” said Duchin. “The entire medical community has to be ready.”
|