Contributed by: Steven J. Rockoff, MD and Diana L. Lam, MD – June 1, 2020
Question 1
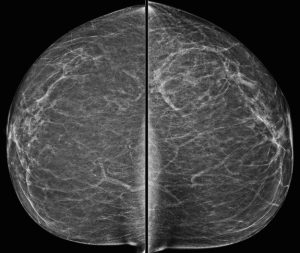
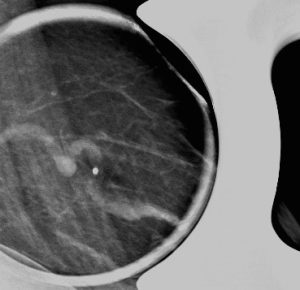
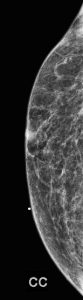
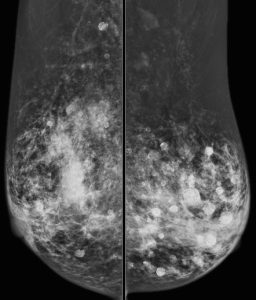
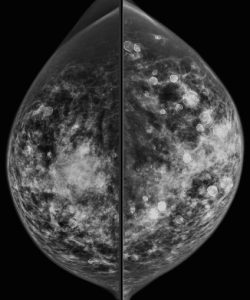
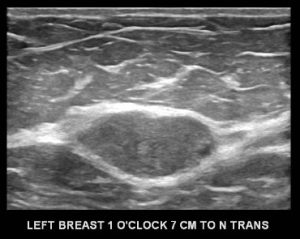
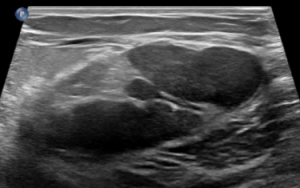
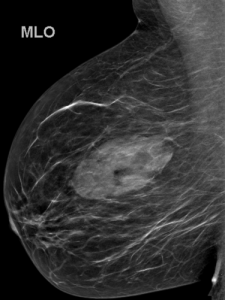
A 43-year-old woman presents for a screening mammogram:


What is the most striking finding?
A. Right axillary lymphadenopathy
B. Marked vascular calcifications
C. Diffuse skin thickening
D. Left nipple inversion
E. Multiple bilateral round and oval massses
Answer
E. Multiple bilateral round and oval massses
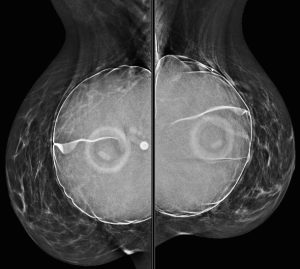
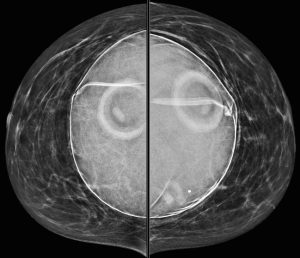
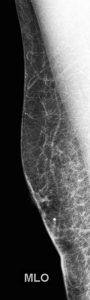
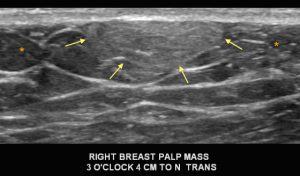
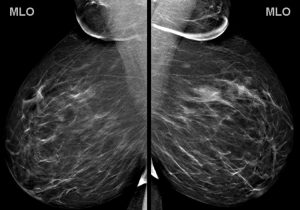
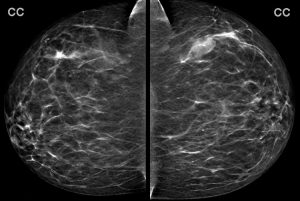
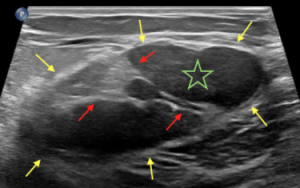
Explanation: There are multiple circumscribed round and oval masses (arrows on the below images). At least two masses are seen in each breast on these 2D images (when scrolling through the tomosynthesis images, even more masses can be seen).
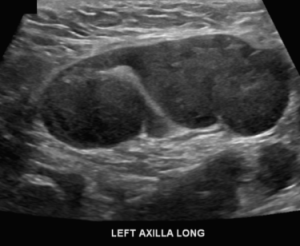
There are no enlarged axillary lymph nodes. There are several skin folds projecting over the axilla on the right MLO image.
There is no nipple inversion or retraction. The left nipple looks like it is behind the skin on the CC image, however this is due to the nipple not being in profile when the image was acquired. Both nipples appear normal and symmetric on the MLO projections.


Question 2
What is your assessment and recommendation?
A. BI-RADS 0 (Incomplete); Recommend diagnostic mammogram and ultrasound
B. BI-RADS 1 (Negative); Recommend one year follow-up
C. BI-RADS 2 (Benign); Recommend one year follow-up
D. BI-RADS 3 (Probably Benign); Recommend six month follow-up
E. BI-RADS 4 (Suspicious); Recommend biopsy
Answer
C. BI-RADS 2 (Benign); Recommend one year follow-up
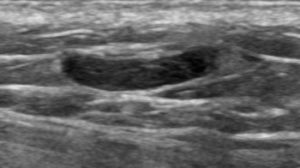
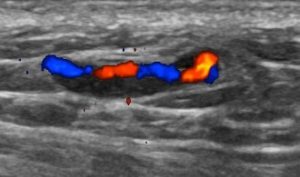
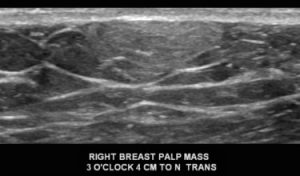
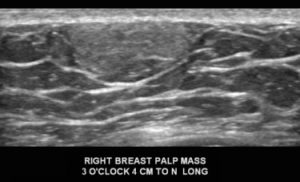
Explanation: There are multiple, bilateral, round and oval, circumscribed, benign-appearing masses. This is a situation for which there is strong data to suggest that there is an essentially 0% likelihood of malignancy. The multiplicity and bilaterality is indicative of multiple cysts, or less often fibroadenomas.
If there are at least three similar benign-appearing masses, with at least one in each breast, then they can be designated benign (BI-RADS 2). No further diagnostic work-up is indicated unless one of the masses appears significantly different from the others or is growing significantly.
In women who have these multiple benign-appearing masses, it can be normal for them to slightly fluctuate in size between yearly exams, as cysts are known to do.