Contributed by: Steven J. Rockoff, MD and Diana L. Lam, MD – June 1, 2020
Question 1
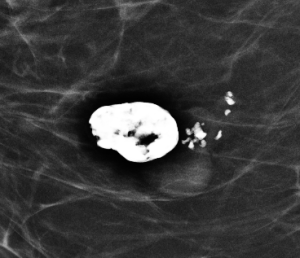
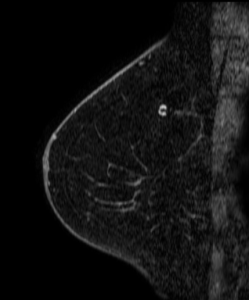
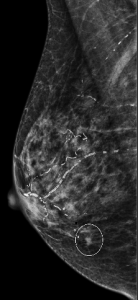
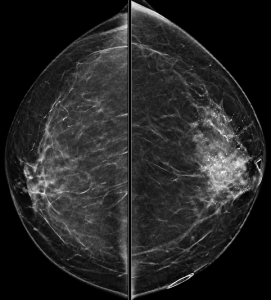
Magnification views were performed for the right breast calcifications seen on a screening mammogram:


What is the best descriptor for this type of calcification?
A. Large rod-like calcification
B. Amorphous calcification
C. Skin calcification
D. Milk of calcium
E. Popcorn-like calcification
Answer
E. Popcorn-like calcification
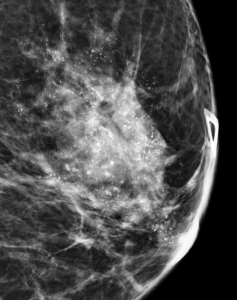
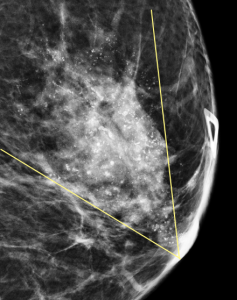
Explanation: These are the large, coalescent, coarse or “popcorn-like” calcifications that are typical of an involuting fibroadenoma.
There are actually probably two or three adjacent fibroadenomas in this location. The dominant large calcification represents the end stage of an entirely calcified involuting fibroadenoma. The smaller adjacent popcorn-like calcifications represent an earlier stage of involution in a different fibroadenoma.
Question 2
What is the best BI-RADS assessment for this finding?
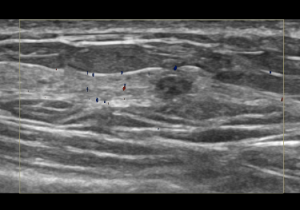
A. BI-RADS 0 (Incomplete); Recommend diagnostic ultrasound
B. BI-RADS 2 (Benign); Recommend one year follow-up
C. BI-RADS 3 (Probably Benign); Recommend six month follow-up
D. BI-RADS 4 (Suspicious); Recommend biopsy
Answer
B. BI-RADS 2 (Benign); Recommend one year follow-up
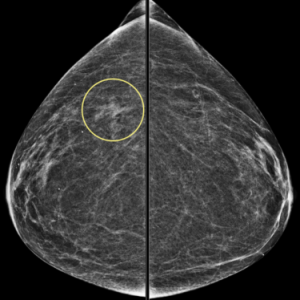
Explanation: A mass with this type of popcorn-like calcifications is almost certainly a fibroadenoma and benign. Having prior mammograms which demonstrate little or no change over time can increase your confidence.
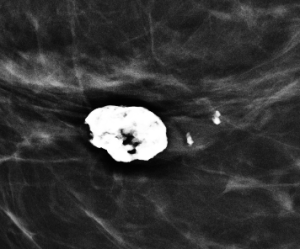
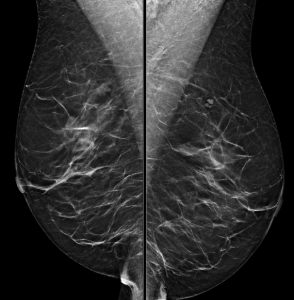
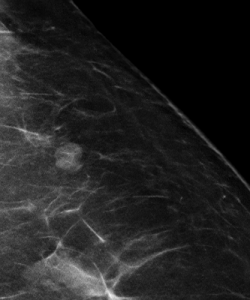
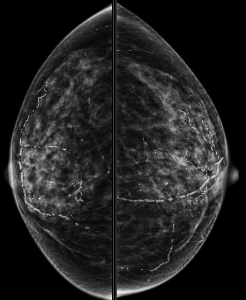
In this patient’s case, there is gradual involution (and slowly increasing calcifications) of this fibroadenoma (image on the left) compared to mammogram five years prior (image on the right):