Contributed by: Steven J. Rockoff, MD and Diana L. Lam, MD – June 1, 2020
Question 1
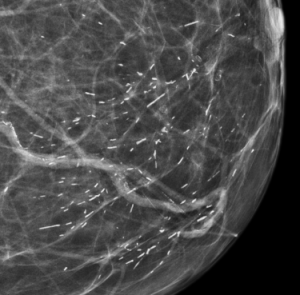
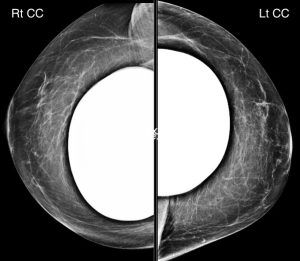
A 63-year-old woman presents for a screening mammogram. She has a history of right breast cancer 10 years ago with treatment that included lumpectomy. The right breast is shown here:


What is the best description for the most concerning abnormality found on this exam?
A. Mass
B. Architectural Distortion
C. Focal Asymmetry
D. Asymmetry
Answer
D. Asymmetry

Explanation: There is an asymmetry in the medial right breast which is seen only on the CC projection, with no MLO view correlate. According to the ACR BI-RADS Atlas, an asymmetry is a unilateral deposit of fibroglandular tissue that does not meet the definition of a mass and is seen on only one mammographic projection (this is in contrast to a focal asymmetry, which is seen on two projections).
There are findings related to prior lumpectomy and radiation in the posterior right breast. With the exception of a slight increase in several benign-appearing dystrophic calcifications, these post-treatment findings are stable compared to last year’s mammogram and not worrisome.
Question 2
After identifying the asymmetry, what is your assessment and recommendation for this screening mammogram (assume the left breast appears normal)?
A. BI-RADS 0 (Incomplete); Recommend diagnostic mammogram and ultrasound
B. BI-RADS 1 (Negative); Recommend one-year follow-up
C. BI-RADS 2 (Benign); Recommend one-year follow-up
D. BI-RADS 3 (Probably Benign); Recommend six-month follow-up
E. BI-RADS 4 (Suspicious); Recommend biopsy
Answer
A. BI-RADS 0 (Incomplete); Recommend diagnostic mammogram and ultrasound
Explanation: The appropriate next step is a diagnostic work-up, starting with a diagnostic mammogram, and following with an ultrasound if the asymmetry persists on the spot diagnostic images. Although a new asymmetry is worrisome, there is a possibility that it represents superimposition of normal fibroglandular tissue, and so it would not be appropriate to jump straight to biopsy.
Question 3
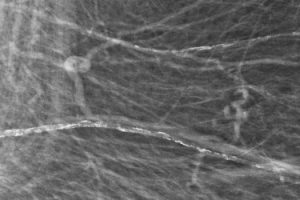
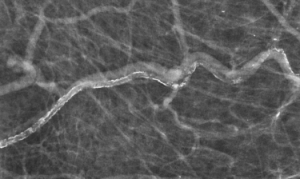
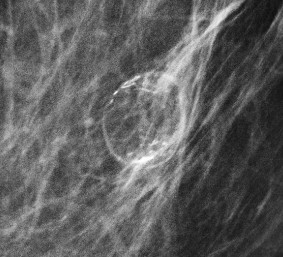
The asymmetry persisted on the diagnostic mammogram and an ultrasound looking for the abnormality in the medial half of the right breast was performed. This is a representative image from the diagnostic ultrasound.

What is your assessment and recommendation?
A. BI-RADS 0 (Incomplete); Recommend MRI
B. BI-RADS 3 (Probably Benign); Recommend six-month follow-up
C. BI-RADS 4 (Suspicious); Recommend stereotactic biopsy
D. BI-RADS 4 (Suspicious); Recommend ultrasound-guided biopsy
Answer
D. BI-RADS 4 (Suspicious); Recommend ultrasound-guided biopsy
Explanation: This irregular mass is suspicious and should be biopsied (BI-RADS 4). When a mass is visible on both ultrasound and mammogram, an ultrasound-guided biopsy is usually preferred over a stereotactic biopsy, as the former option is usually more comfortable for the patient and allows for real-time visualization of the target by the performing physician. Additionally, there may be technical challenges in performing stereotactic biopsy on a far posterior mass such as this one.