November 27, 2018
November 2018 Newsletter

Carlos A. Pellegrini, MD, FACS Chief Medical Officer, UW Medicine and Vice President for Medical Affairs
In a month when we pause to reflect on what we are thankful for, I am honored every day to witness all your hard work to serve our mission — to improve the health of the public — and help accomplish the UW Medicine Way. Some work is iterative – improving or growing transformative programs, while some is in early stages and unfinished. November is Lung Cancer Awareness Month and this issue of our newsletter highlights the expansion of a screening program that will help save lives. But, for me, there is no more important unfinished work than the work around healthcare equity. To that end, I invite you to join me and your colleagues in reading and engaging in a community conversation around a book that will help us advance our healthcare equity agenda. The book is Ijeoma Oluo’s “So You Want to Talk about Race” and I hope you’ll take the time to read it over the next few weeks. This is a thoughtful and engaging bestselling book by a local author aiming to help us all have better conversations on equity, diversity and inclusion. This book and the community conversation we hope to have about it is just one aspect of our healthcare equity agenda and I encourage you to find out more on our newly refreshed healthcare equity website (read more below). Thanks for all you do and I wish you a happy start to the holiday season.
Early Screening Pilot Key to Lung Cancer Survival

Lung cancer is the second most common malignancy among men and women in the U.S., and is responsible for more deaths than breast, prostate, and colorectal cancer combined. Despite decades of advances in science and medicine, overall survival rates for lung cancer have improved only marginally. This is due in large part to a prominence of late-stage presentation. An important breakthrough published in 2011 proved that annual screening with low-dose computed tomography (LDCT) leads to a 20% reduction in lung cancer mortality among high-risk individuals. In order to reap the benefits of this simple, quick, safe, and non-invasive test, more eligible individuals need to be offered lung cancer screening. One of the greatest challenges facing health systems now is providing greater access to this life-saving test.
Seattle Cancer Care Alliance (SCCA) through its Lung Cancer Early-Detection and Prevention Clinic (LCEDPC) — staffed by pulmonary physicians and providers — began a screening program for high-risk patients in 2012, along with shared decision-making and tobacco cessation services. According to the United States Preventive Service Task Force, high-risk individuals are considered to be:
- People aged 55-80 years of age
- Current or former smokers (who quit within last the last 15 years)
- People with at least a history of smoking 30 or more “pack years”
The SCCA LCEDPC also created a provider-facing pop-up alert for individuals identified as high-risk for lung cancer within the electronic health record (EHR), and a “smart set” to facilitate ordering of screening services in Epic.
With a high level of evidence supporting lung cancer screening, it is now recommended as a preventative measure and covered by Medicare, Medicare Advantage, Medicaid, commercially insured individuals (including ACN and value-based contracts), and eligible individuals paying out-of-pocket. In September of this year, UW Medicine took an important step in advancing a population health management approach to lung cancer screening, spearheaded by Farhood Farjah, MD MPH.
“We wanted to take a comprehensive approach that would result in increased lung cancer screening rates,” said Farjah. “Working as a team with primary care, specialists and patients themselves is the best path toward achieving that goal.”
Led by PATH (Population Approach to Health) Program manager Nkem Akinsoto, MSc, the centralized population health management team developed a three-pronged model to assist in patient identification, education/outreach and clinician engagement.
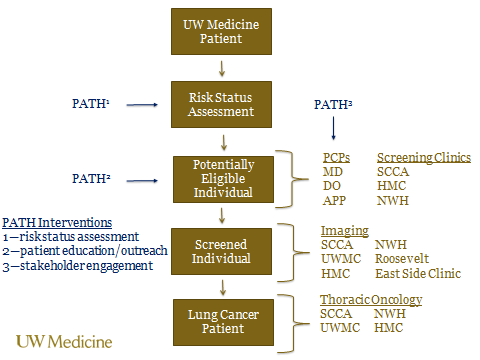
The first step was to identify patients with missing risk factor information (smoking status, pack-years of exposure, years since quitting) within the EPIC system. The PATH team then reached out to those patients via letters and follow-up phone calls to obtain additional risk information, which was recorded in Epic, enabling pop-up identification alerts when appropriate.
The second step was to reach out to patients who were confirmed to be high-risk in order to provide education on screening details and encourage shared decision-making visits, LDCT, and smoking cessation resources as needed.
The third aspect of the PATH initiative is engagement for primary care teams including awareness of screening resources in the system, instruction on proper coding and “smart set” orders, and the collaborative design of dashboards intended to provide performance feedback measures of screening utilization in eligible patients.
Work is continuing to schedule screenings and shared-decision making visits not already set up, obtaining missing or incomplete data of patients to enter into the EHR and determine additional eligible high-risk individuals, and identification and outreach of newly eligible patients in the system.
“The PATH initiative is a win-win for all — patients, providers, and the health system,” said Farjah.
Briefly
- To help us further advance the objectives of our healthcare equity blueprint, we want to provide information, awareness and resources on our efforts and programs. The healthcare equity website was designed to be a source of that information and was recently refreshed to include details on our Transgender and Gender Non-Binary (TGNB) Care Program. Our UW Medicine Healthcare Equity Toolkit was also rolled out. This toolkit is designed to be a resource to support and guide UW Medicine leaders and staff in our effort to embrace diversity, foster inclusion and advance equity for our patients and workforce. Within this toolkit you will find:
- A guide to convening a local (entity or department) equity, diversity and inclusion (EDI) committee
- A glossary of EDI terms
- A calendar of cultural observances and celebrations
- Reading, audio and video EDI resources
- A list of internal and external EDI training resources
- Information that covers topics such as ableism, ageism, citizenship, LGBTQ, and race/ethnicity
- For questions or feedback, reach out to: hcequity@uw.edu