[Skill Modules
>>
Heart Sounds & Murmurs
>>
Techniques
]
Technique: Heart Sounds &
Murmurs
Using the Stethoscope
A modern stethoscope consists of two earpieces connected by tubing to a chest piece which usually has both diaphragm and bell attachments. Earpieces should be angled forwards to match the direction of the practitioner's external auditory meati.
The bell is used to hear low-pitched sounds. Use for mid-diastolic murmur of mitral stenosis or S3 in heart failure.
The diaphragm, by filtering out low-pitched sounds, highlights high-pitched sounds. Use for analyzing the second heart sound, ejection and midsystolic clicks and for the soft but high-pitched early diastolic murmur of aortic regurgitation.
back to top
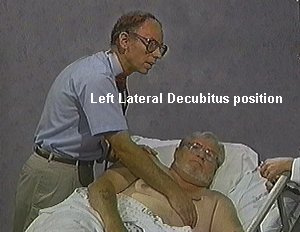
Positioning the Patient
Patients can be examined while lying supine, in the left lateral decubitus position (see picture) and sitting, leaning forward.
Pericardial sounds are sometime best heard with the patient on hands and knees.
back to top
Examination
1. Auscultate the heart at various sites
- At the apex.
- At the base (the part of the heart between the apex and the sternum)
- In the aortic and pulmonary areas to the right and left of the sternum, respectively
Listen for normal heart sounds:
-
The 1st heart sound, S1 (lub), marks the beginning of systole (end of systole).
- Related to the closure of the mitral and tricuspid valves.
- Loudest at the apex.
-
The 2nd hear sound, S2 (dub), marks the end of systole (beginning of diastole).
- Related to the closure of the aortic and pulmonic valves.
- Loudest at the base.
You can relate the auscultatory findings to the cardiac cycle by simultaneously palpating the carotid artery while listening to the heart:
| S1 |
S2 |
| Just precedes carotid pulse |
Follows carotid pulse |
| Louder at apex |
Louder at base |
| Lower pitch and longer than S2 |
Higher pitch and shorter than S2 |
|
Because systole is shorter than diastole:
|
| First of two grouped beats |
Second of 2 grouped beats |
If anything abnormal is found, move the stethoscope around until the abnormality is heard most clearly.
2. Separate findings into six categories
- 1st & 2nd Heart Sounds
- 3rd & 4th Heart Sounds
- Clicks & Snaps
- Murmurs
- Rubs
- Maneuvers
3. Analyze each category individually and then put it together to diagnosis the problem
| Category |
Definition |
Audio examples |
|
Aortic stenosis:
|
Murmur:
- Harsh late-peaking crescendo-decrescendo systolic murmur
- Heard best- left 2nd ICS
- Radiation to the carotids.
Possible associated findings:
- Abnormal carotid pulse
- Diminished and delayed ("pulsus parvus and tardus")
- Sustained Apical impulse
- Calcified aortic valve on CXR
|

 |
|
Mitral Regurgitation:
|
Murmur:
- Blowing holosystolic murmur
- Heard best at the apex
- Radiation to the axilla and inferior edge of left scapula.
Possible associated findings:
- S2:
wide physiologic splitting
- S3
|
 |
|
Aortic insufficiency:
|
Murmur:
- Soft blowing early diastolic decrescendo murmur
- Heard best at the left 2nd ICS without radiation
- May also hear systolic flow murmur and diastolic rumble (Austin Flint)
Possible associated findings:
- Dilated apical impulse
- Abnormal and collapsing arterial pulses
|
 |
|
Tricuspid regurgitation:
|
Murmur:
- Soft holosystolic murmur
- Heard best at the LLSB without radiation
- Intensity increases with inspiration or pressure over liver
Possible associated findings:
- Elevated neck veins
- Systolic regurgitant neck vein
- Systolic retraction of apical pulse
- Edema, Ascites or both
|
|
|
Pulmonic Insufficiency
|
Murmur:
- High frequency early diastolic decrescendo murmur
- Heard best at 2nd-3rd ICS
- Increases with inspiration
Associated findings:
- Abnormal S2
splitting
- Sustained pulmonary hypertension
|
|
| Pulmonary stenosis |
Murmur:
- Harsh crescendo-decrescendo systolic murmur
- Heard best sternal border bat 2nd or 3rd intercostal spaces
- Increases with inspiration
Associated findings:
- Ejection sounds heard at sternal edge, 2nd or 3rd intercostal space
- Wide physiological splitting of S2
- Prominent A wave of the jugular venous pulse
|
 |
|
Mitral stenosis
|
Murmur:
- Low frequency rumbling mid-diastolic murmur, with presystolic component
possible
- Heard best at apex
- Accentuated in left lateral decubitus position
Associated findings:
- Apical impulse absent or small
- Irregular pulse ( atrial fibrillation)
- Loud S1
- Elevated neck veins with exaggerated A wave
|
 |
|
Hypertrophic cardiomyopathy
|
Murmur:
- Harsh quality midsystolic murmur
- Heard best LSB
- Increases with decreased venous return
Possible associated findings:
- Sustained apical beat to palpation
- S4 (50% of the time)
|
|
|