
The Program to Encourage Active, Rewarding Lives or PEARLS has been proven effective in treating depression for older adults. A recent PEARLS study also shows promising data about addressing social isolation and loneliness.
Evidence-based programs, such as PEARLS, have been rigorously tested in controlled settings, proven effective in multiple settings, and translated into practical models that can be delivered in community and clinical settings outside of the research study.
PEARLS is designed to take into account the real-world strengths and challenges organizations face when delivering the program, such as staffing and competing priorities.
The University of Washington Health Promotion Research Center and its community partners have collaborated on various PEARLS research projects, including research that developed the program and tested its effectiveness. The center and its partners also research how to adapt, deliver, and sustain PEARLS.
Treating Depression
During a community-engaged randomized controlled trial from 2000 to 2003, researchers tested the effectiveness of PEARLS in treating depression for older adults. Findings from this study show PEARLS is an effective treatment for managing depression among older adults.
No clinical diagnosis is needed for older adults to participate PEARLS, although organizations do screen potential participants for depressive symptoms.
Study Participants
The older adults who participated in the 2000-2003 study had clinically significant depressive symptoms suggestive of depression or persistent depressive disorder (a chronic form of depression).
- Mean Age: 73
- Race & Ethnicity: 42% people of color
- Living Alone: 72%
- Low-Income*: 58%
- Chronic Conditions: 4-5 conditions on average
* Less than $10,000 household income
Findings
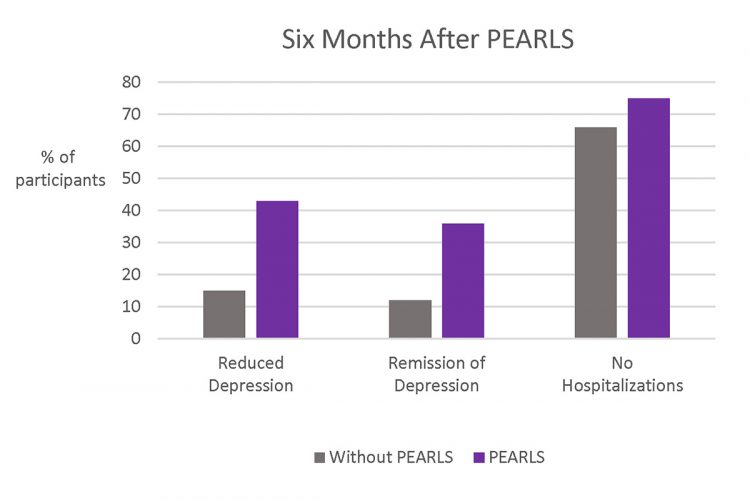
Six months after older adults participated in PEARLS, they were more likely to experience the following than those who did not participate in PEARLS:
- Have a 50% or greater reduction in depression symptoms.
- Achieve complete remission from depression symptoms.
- Trend toward lower hospitalization rates (this includes any type of hospitalization, not just those related to mental health).
- Have greater health-related, quality-of-life improvements in both functional well-being (e.g., improved sleep or ability to work) and emotional well-being (e.g., less nervous or worried about health conditions).
PEARLS Evidence: Treating Depression
Community-Based Treatment of Late Life Depression an Expert Panel-Informed Literature Review
This project was a systematic literature review where investigators found that both clinic- and community-based depression care management programs, such as PEARLS, are effective for treating late-life depression.
LEARN MORE
Recommendations for Treating Depression in Community-Based Older Adults
Experts in the fields of mental health, public health research, and community practice created recommendations for community-based treatment of late-life depression for public health and aging networks. This included programs such as PEARLS.
LEARN MORE
Treating Depression in Older Adults: Challenges to Implementing the Recommendations of an Expert Panel
This paper describes real-world experiences in implementing evidence-based interventions, such as PEARLS, in various community settings. The article highlights partnerships with older adults, providers, and policymakers to overcome challenges to funding, training, and delivering depression care.
LEARN MORE
PEARLS Evidence: Depression & Epilepsy
PEARLS Depression Treatment for Individuals With Epilepsy: A Randomized Controlled Trial
Individuals with epilepsy who participated in PEARLS were more likely to experience lower depression severity and suicidal ideation as well as better emotional well-being, as compared to those who did not participate in PEARLS.
LEARN MORE
Long-Term Outcomes From the PEARLS Randomized Trial for the Treatment of Depression in Patients With Epilepsy
PEARLS significantly reduces depressive symptoms in adults with epilepsy. People were able to maintain that reduction for more than one year after completing the program.
LEARN MORE
Addressing Social Isolation & Loneliness

While social isolation and loneliness can be connected, they are different. Social isolation is physically being alone or separated from other people or services. For example, social isolation can happen while in a rural community, living away from family as an older immigrant, or someone is home-bound. Loneliness is the feeling of being alone, regardless of the amount of social contact or interaction someone has. While social isolation can cause someone to feel lonely, people can also feel lonely when they are around others.
Because social isolation and loneliness are different, they require different approaches. PEARLS supports staff at community-based organizations in understanding how to identify the cause of someone’s depression, social isolation, and/or loneliness, as well as collaborating with them on how to address their unique situation. For example, if someone is lonely while living in a group home around others, spending more time around people might not address their issue. But working on how to develop deeper, more meaningful relationships with a select few could help.
In collaboration with 15 community-based social service organizations across five states, we evaluated whether older adults were able to decrease their social isolation and loneliness after participating PEARLS. This project, known as PEARLS Connect, was from 2017 to 2021 and made possible thanks to funding from the AARP Foundation.
Study Participants
We intentionally partnered with organizations that engage older adults with diverse backgrounds who were experiencing poverty and depression.
- Mean Age: 73
- Race & Ethnicity: 21% Black, 19% Latino, 4% Asian or American Indian/Alaskan Native
- Language: 15% Spanish-speaking
- Living Alone: 61%
- Low-income*: 81%
- Chronic Conditions: 43% had five or more
* Below 250% of the Federal Poverty Level
Findings
After participating in PEARLS, older adults significantly improved in the three measures of social isolation and loneliness:
- Social Interactions & Satisfaction With Social Support
Measurement Tool: Duke Social Support 10-item Questionnaire - Perceived Social Isolation
Measurement Tool: Patient-Reported Outcomes Measurement Information System for Social Isolation 6-item Questionnaire (PROMIS-SI-6 item) - Loneliness/Reduced Loneliness
Measurement Tool: UCLA 3-Item Loneliness Questionnaire
This study took place before and during the COVID-19 pandemic (2017-2021). Overall, PEARLS participants improved their social connectedness (feeling that you belong to a group and are close to other people) even during early the early months of the pandemic (data was collected through May 2020). But their improvements in social interactions (e.g., number of social activities) were no longer scientifically significant. This is likely because of COVID-19 restrictions, such as stay-at-home orders, that changed how and if people were able to safely socialize and interact with others.
We are analyzing our latest interviews and surveys for this project. We will share more findings when they are ready.

Dissemination & Implementation
We also study how to spread information about PEARLS as well as how organizations can improve implementation and use of the program.
PEARLS Evidence: Dissemination & Implementation
Implementation of an Evidence-Based Depression Care Management Program (PEARLS): Perspectives From Staff & Former Clients
Researchers conducted focus groups with PEARLS participants, providers, managers, and referrers to identify program benefits. They also identified unintended consequences, facilitators, and barriers to program delivery, along with strategies for addressing these issues.
LEARN MORE
Translating PEARLS: Lessons Learned from Providers & Participants
We have learned a lot from organizations and staff that deliver PEARLS through our monthly technical assistance calls and other dissemination and implementation research and activities. We have also learned a lot from program participants through PEARLS sessions, focus groups and interviews. A selection of key learnings is provided in this publication, organized by Glasgow’s RE-AIM framework to help improve the success of evidence-based program delivery in real-world settings. It is important for programs to perform well across each of the five elements of the framework – reach, adoption, effectiveness, implementation, maintenance – in order to maximize overall impact.
LEARN MORE
Development & Evaluation of a Fidelity Instrument for PEARLS
This publication describes the development and the preliminary evaluation of a fidelity instrument for PEARLS. Our findings suggest that providers may be able to use the instrument to assess the fidelity of PEARLS in various settings across the country.
LEARN MORE
It Could Be a Pearl to You: Exploring Recruitment & Retention of PEARLS With Hard-to-Reach Populations
Researchers interviewed PEARLS participants, providers, and referrers from community-based organizations to better understand how to reach underserved populations. Communities in this project included veterans, African Americans, Filipino men, immigrants and English-language learners, rural community members, and people with limited education. The themes of trust, cultural appropriateness, meet them where they are, and framing and reframing, cut across barriers to participation in PEARLS and approaches for overcoming these barriers.
LEARN MORE
Development & Evaluation of a Peer-Driven Engagement Intervention to Reach Older Veterans With Depression
Researchers trained PEARLS graduates who were military veterans, or partners of veterans, to provide outreach about PEARLS to their peers in the veteran community.
LEARN MORE