
PEARLS is an effective skill-building program that helps older adults manage and reduce their feelings of depression and isolation. Some older adults might also describe those feelings as chronic sadness, loneliness, frustration, being overwhelmed, or losing interest in things they love.
PEARLS adapts to the participant and the place and the need. The program is used by numerous cultures and communities. By removing barriers related to race, poverty, and where someone lives, PEARLS makes mental health services more available to underserved communities. Sessions with older adults take place in their homes or other community-based settings that are more accessible and comfortable for older adults.
PEARLS is simple and easy to administer by staff at community-based organizations who might not have previous counseling experience or a higher education. There is PEARLS training that prepares staff to provide the program to community members.
PEARLS Coaches

PEARLS coaches are the heart and soul of an organization’s PEARLS. They are the staff at community-based organizations who meet one-on-one with older adults to help them build the skills they need to live happier, healthier, and more independent lives. PEARLS coaches are a participant’s support, cheerleader, and connection to resources.
This close partnership between a PEARLS participant and coach builds throughout the six to eight one-hour PEARLS sessions. These sessions occur over the course of four to five months, starting with weekly sessions and tapering to monthly. This is a common skill-building technique used to support people in gradually learning to problem solve on their own.
We provide training to become a PEARLS coach, as well as ongoing support for coaches.
PEARLS Reach
National
12,838+ older adults
211 organizations
35 states + D.C.
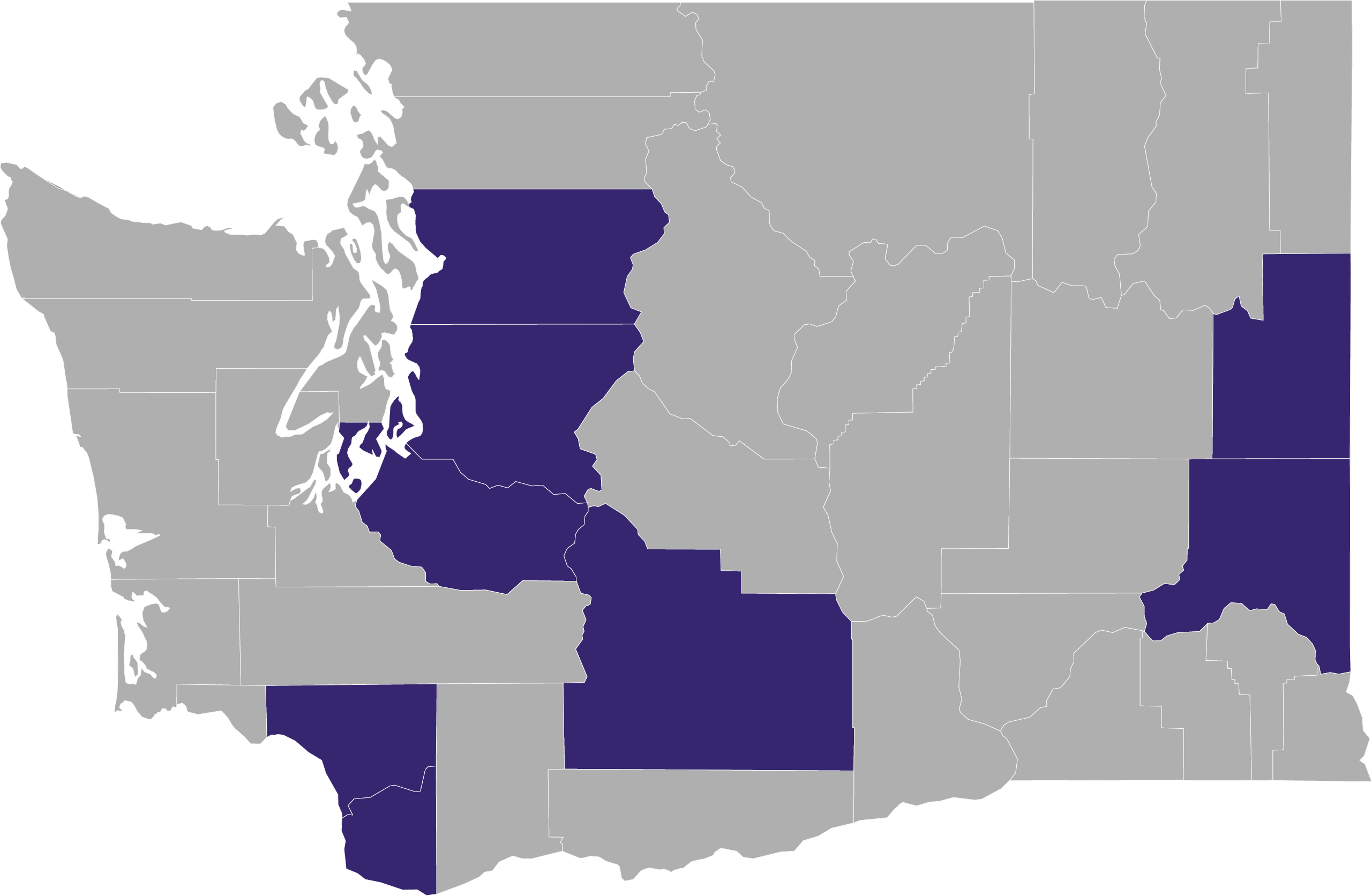
Washington State
2,150+ older adults
17 organizations
8 counties
Our Partnerships
Partnerships with community-based organizations and organizations that providing funding for programs such as PEARLS are what make this program possible.
Here is what a few of our partners had to say about our collaborative efforts with PEARLS.
“I see the UW Health Promotion Research Center as our personal cheerleaders. They celebrate our accomplishments with us and help us troubleshoot when we are struggling.”
Amelia, El Sol Neighborhood Educational Center
(San Bernardino, California)
“With the UW Health Promotion Research Center, we feel more confident. They enable us and empower us to continue our linkages with older folks and our veterans.”
Sluggo, Filipino Senior & Family Services
(Seattle, Washington)
“The UW Health Promotion Research Center partnership provides accessible, non-judgmental support and expertise. They engage and brainstorm with us on ways to reduce barriers to offerings in our rural communities.”
Susan, Rogue Valley Council of Governments Senior & Disability Services
(Central Point, Oregon)
“I really appreciate the UW Health Promotion Research Center’s understanding and flexibility when my clients have their own unique challenges and needs. The UW partnership and programs have been very effective among people with different cultural and linguistic backgrounds, including in our community.”
Syed, Union for Pan Asian Communities
(San Diego, California)
Frequently Asked Questions (FAQs)
Learn a little more about the Program to Encourage Active, Rewarding Lives (PEARLS) and how it works. We have divided questions into three categories, although some questions and responses may overlap.
- Overview of PEARLS: These are questions people often have when exploring PEARLS as an option for their organization and community.
- Providing PEARLS in Your Community: These are questions people often have about what to expect when providing PEARLS or questions they have about providing the program.
- Spreading the Word About PEARLS: These are questions people have about promoting or sharing PEARLS information with their community and potential PEARLS participants.
Please note: We refer to staff at community-based organizations who provide PEARLS to older adults as PEARLS coaches, although organizations can adapt this term to what works best for their community.
Overview of PEARLS
These are questions people often have when exploring PEARLS as an option for their organization and community.
What is PEARLS?
PEARLS is an evidence-based program that helps older adults with depression create happier, healthier lives. The program educates older community members about what depression is (and is not) and helps them develop the skills they need for self-sufficiency and more active lives. PEARLS offers a home or community-based setting that is more accessible and comfortable for older adults who do not see clinical mental health programs as a good fit for them, while also allowing for coordination with their current health care providers.
PEARLS Is Flexible & Adaptable to Community Needs
It is adaptable to various community needs and helps expand access to depression care in underserved communities, including rural ones. It is a program for all older adults, especially those who have limited access to depression care because of systemic racism, trauma, language barriers, low income, and/or where they live. This is because PEARLS was designed in collaboration with the organizations that deliver it, validated in partnership with the communities who use it, and adaptable to the people who need it.
No Diagnosis to Participate in PEARLS
Older adults do not need be diagnosed with depression in order to participate in PEARLS. Organizations screen potential participants for depressive symptoms using tools we can provide.
No Counseling Experience or Higher Education to Provide PEARLS
PEARLS is simple and easy to administer by staff at community-based organizations who might not have previous counseling experience or a higher education. There is PEARLS training that prepares staff to provide the program to community members.
Short-Term Sessions With Results
PEARLS coaches (the name we give frontline staff at community-based organizations providing the program) meet one-on-one with older adults for six to eight one-hour sessions, typically over the course of four to five months. The program begins with weekly sessions that gradually taper to monthly. This is a common skill-building technique used to support people in gradually learning to problem solve on their own.
Training & Support Provided by UW
The University of Washington Health Promotion Research Center (UW HPRC) provides long-standing and deeply rooted support for PEARLS, including its establishment as an evidence-based program. Our center has supported PEARLS from its early development. We are committed to its success. We offer several training opportunities each year, and those who have completed training are eligible to participate in free, ongoing support such as monthly technical assistance calls with us and other organizations around the country that are providing PEARLS.
PEARLS Training
How is PEARLS different from other depression programs?
PEARLS is one of only a handful of programs that focuses on helping older adults develop the skills they need to maintain their health, happiness, and independence. The program is part of a cultural shift in how depression is managed by and for aging community members. Most programs address depression in older adults using only the clinical mental health toolkit (counseling and/or medication).
PEARLS was designed in collaboration with the organizations that deliver it, validated in partnership with the communities who use it, and adaptable to the people who need it. Support offered through the program is tailored to the individual needs of older adults. The program itself is designed for use by non-clinical, community-based organizations serving communities that have limited access to clinical care.
Which communities have had success with PEARLS?
It is adaptable to various community needs and helps expand access to depression care in underserved communities, including rural ones. It is a program for all older adults, especially those who have limited access to depression care because of systemic racism, trauma, language barriers, low income, and/or where they live.
PEARLS recognizes that different communities celebrate their elders in different ways and is designed to build on those strengths. This is because PEARLS was designed in collaboration with the organizations that deliver it, validated in partnership with the communities who use it, and adaptable to the people who need it.
The UW Health Promotion Research Center continues to build and expand its PEARLS partnerships, which are key to the success and effectiveness of the program.
Some PEARLS materials have been translated in Somali, Russian, Spanish, and Chinese. The questionnaire used to measure individual progress during PEARLS sessions (known as the PHQ-9) is offered in more than 80 languages. We can provide copies and links to additional materials, although we also recommend reviewing translated materials with native speakers from the community to ensure that the language is appropriate.
Organizations have provided PEARLS to older adults who have also been receiving other mental health or addiction services, and with participants who are on medication. Additional therapies and services should be provided outside the PEARLS session and with a staff member or partnering organization that is not the participant’s PEARLS coach.
What we have learned about working with some populations and health situations through PEARLS research and ongoing assistance activities:
- Military Veterans & Their Partners: Aging and Disability Services in King County, Washington has had much success using PEARLS to support veterans and their partners. Recruitment and mental health stigma may be a barrier, but we encourage building a strong rapport with your local veteran community and its members.
- Racial & Ethnic Communities: PEARLS has been successfully implemented through agencies that focus on specific racial and/or ethnic populations. Having a PEARLS coach that is from the same or similar cultural background as a participant is helpful but not required. If that is not possible, having a community representative who can build a bridge between the coach and the participant is another option, as is providing cultural humility and cultural competency training for staff.
- LGBTQIA Community Members: The LGBTQIA community has benefited from PEARLS, especially those who may be isolated and face stigma as a LGBTQIA community member. They may also be experiencing the loss of a partner and no adult children, which can add to their isolation, loneliness and/or depression.
- Rural Communities: These communities tend to have fewer transportation options and can be more isolated, including limited access to internet. Meeting older adults in their homes can be a huge advantage of PEARLS in rural areas, because the coach can provide a connection to additional community services that might be difficult for isolated older adults to access. Although we do recommend that some sessions take place in the home or community setting, it is also possible to provide PEARLS sessions over-the-phone.
- Low-Literacy: A PEARLS coach can read worksheets aloud and may have a caregiver help an older adult fill out worksheets, as long as the caregivers or coach does not make decisions on behalf of the PEARLS participant.
- Mild Cognitive Impairment: This may not be grounds for exclusion from PEARLS if a participant is still able to focus during the session and complete goals. Participants can engage caregivers to assist with activities, but it is essential the caregiver not do the activity for the participant.
- Mental Illness: PEARLS has been beneficial to those with bipolar or other mental illnesses if they are managing their condition and/or on medication so that they are able to focus during the session and complete goals.
- Substance Use: PEARLS has been beneficial to those with substance use disorder if they are managing their condition so that they are able to focus during the session and complete goals.
It is most important that the older adult is able to make decisions and be involved in the PEARLS process. Participants need to be able and willing to engage. Engagement activities can be minor and easy to accomplish. Adaptions to meet individual needs can also be done, such as having a PEARLS coach read documents to the participating older adult and fill out forms under the direction that older adult (this could be for people who are blind and/or people with limited English skills).
Which organizations have had success with PEARLS?
PEARLS is designed to be delivered by staff at community-based organizations who can visit older adults in their homes or in community settings that are outside of traditional mental health settings. PEARLS has also been implemented at community mental health agencies.
More than 9,400 older adults and 133 organizations across 26 states have participated in PEARLS.
PEARLS has been successful at organizations that support underserved communities.
Organizations that have the most success with the program are ones where PEARLS aligns with its mission.
See what some of our partners have to say about our work together.
Our Partnerships
To see some of the organization that offer PEARLS, check the Evidence-Based Leadership Collaborative (EBLC) Map of Programs. You will need to filter by program and select PEARLS. Please note, that is not a complete list of all the organizations offering PEARLS.
How do I know if PEARLS is a good fit for my organization?
To answer this question, you will need to ask, “Does PEARLS align with my organization’s mission?”
If your organization’s mission includes these factors, PEARLS could support your efforts:
- Improving health (including behavioral health)
- Focusing on the most common issues that older people face
- Empowering participants to direct their own recovery by teaching them self-management skills
What are some benefits and challenges to seeing older adults in their homes (the PEARLS model)?
There are benefits and challenges to seeing older adults in their homes. Knowing both the benefits and challenges will help your organization decide if the program is a good fit. Knowing the potential challenges to visiting people in their homes will also allow you to brainstorm and consider solutions.
Benefits
- A place where participants are comfortable and feel more in control
- Participants don’t have to go anywhere (minimized barriers to accessing services)
- No stigma of going to a therapist’s office
- Connect the participant to the outside world via the PEARLS coach
- Allows you to see the participant in their home environment and get a more holistic picture (e.g. photos of their grandchildren, bare cupboards, fall risks, possible hoarding); this can also help you better understand what existing supports they have available
Challenges
- Travel time required by a coach, which can limit the number of people they see in a day
- Some participants might be reluctant to have someone enter their home (e.g., people with hoarding issues or family members who feel threatened by the older adult working on issues with someone like a PEARLS coach)
- Some home settings are unsafe or difficult to visit (e.g., homes with pest infestations, cigarette smoke, strong odors, etc.)
In challenging situations related to home visits, meeting in community settings where you can have privacy and the participant feels comfortable could be another option.
Can PEARLS be done with current clients or do we need to recruit new ones?
You do not necessarily have to recruit new clients to provide PEARLS. Your agency may already be reaching more isolated community members or those experiencing depression (a clinical diagnosis is not needed) with your other programs and services. PEARLS can help your organization expand or enhance current services you already provide.
With PEARLS, communities have the tools to recognize and respond to depression as an illness that can be treated and managed. Many community-based organizations describe high levels of depression and social isolation among the older adults they serve. This should not be accepted as a normal part of aging.
If your organization is not already serving people who can benefit from PEARLS, you will need to partner with organizations that support underserved older adults, such as Meals on Wheels, senior service agencies, or visiting nurse associations.
We can provide more details and support for recruitment as needed. You can also find information about marketing materials in the FAQs section for “Spreading the Word About PEARLS.”
A clinical supervisor is required for PEARLS. Who can be one?
Clinical supervision is required for PEARLS and is beneficial during challenging cases, stagnant periods for a participant’s progress, and behavioral issues.
When a program first begins, clinical supervisors can review training materials and practice PEARLS techniques with the PEARLS coach. After PEARLS sessions pick up, PEARLS coaches can work with the clinical supervisor to discuss whether a person referred to PEARLS is appropriate for the program, discuss how to support participants who are not improving their depression, recommend medication management if needed, and other services or support.
Who has been a clinical supervisor for PEARLS?
- Psychiatrists
- Psychiatric nurse practitioners
- Licensed clinical social workers (MSW/LCSW)
- Geriatricians or other primary care providers
Clinical supervision can be done over the phone or video conference so the clinical supervisor does not have to be local. If possible, we recommend group supervision where one clinical supervisor meets with multiple PEARLS coaches (from your organization or with coaches from other organizations). This can provide peer learning and support, along with knowledge from the clinical supervisor. It can also potentially save time and money.
We know it can be challenging to obtain psychiatrist services because of limited funding and/or availability. Ideas for connecting with psychiatrists include contacting an academic medical center or university that has training as part of their mission.
What makes a good clinical supervisor for PEARLS?
Know what to look for in a clinical supervisor who is best suited for PEARLS.
- Experience working with depression and other common medications or medical conditions for older adults
- Knowledge of the PEARLS model (participant driven, Problem-Solving Treatment, and Behavioral Activation)
- Capability of understanding cultural issues, responses, and adaptions
- Ability to not stray away from PEARLS techniques
It is okay to have two people providing clinical supervision if needed to fill areas of expertise. For example, some programs use clinical social workers or psychologists for PEARLS supervision and meet less frequently with a primary care provider to review medications.
How often will the clinical supervisors be needed?
It may be helpful to have more than one clinical supervisor, depending on their availability.
- 90-minute sessions 1x/month for small caseloads
- 90-minute sessions 2x/month when caseloads picks up
What should you expect with cost and funding for a clinical supervisor?
A contract is helpful in order to establish supervision goals, hours, and rates. It also makes clear that PEARLS clinical cases are not part of the supervisor’s clinical responsibility.
Rates for a clinical supervisor may vary locally from $150-200 an hour. Look into funding opportunities with organizations and county agencies that work with older adults.
We provide more details about PEARLS funding options in these FAQs.
What is the cost of providing PEARLS and funding options?
This varies depending on how much your staff time costs to deliver the program (factoring in time for recruitment, transportation, and time with the clinical supervisor), whether they are working part-time or full-time to deliver PEARLS, and how much the clinical supervisor’s time costs.
A general estimate is $1,350 or a $150 unit rate for nine sessions (eight in-person sessions, along with one screening and follow-up). This is based on the unit rate that the state Medicaid waiver uses in Washington, as well as what we’ve learned from several other programs.
Time Estimates
This does not include the six to eight PEARLS sessions.
- Clinical Supervision: 1 – 4 hours per month per PEARLS coach/not per participant (each participant is usually only covered a few times during supervision)
- Program Supervision: 1 – 4 hours per month per PEARLS coach (many programs meet with a program manager and other coaches or counselors on a regular basis)
- Travel Time: Calculated per PEARLS participant. Travel time is difficult to estimate because the distance and/or traffic between the PEARLS coach and participant varies greatly, along with how frequently they are meeting (e.g., they may meet for four hours in the first month for weekly visits, but switch to meeting one hour per month)
- Paperwork: 15-30 minutes per PEARLS participant per session (this also depends on the organization’s requirement for entering information into a data management system)
- Recruitment: This is more per PEARLS coach (or program staff in some cases) than per participant. Recruitment can be 1-4 hours per week on presentations, meetings with clinics and/or community-based organizations, etc. Time can also depend on whether you already have relationships with referral organizations or partners.
- Screening: 1 hour per potential participant (a depression diagnosis is not needed)
Potential Funding Sources
- Grants
- Foundations
- Older Americans Act (OAA):
Title III Part D Disease Prevention and Health Promotion (III-D) - Tax Levies
- E.g., Veterans, Seniors & Human Services Levy (King County, Washington)
- E.g., Mental Health Services Act (California)
- Direct Billing or Fee-for-Service Payments
- Medicaid or Medicaid Waiver
When providing information to organizations for funding and grant applications, include as much PEARLS evidence as possible. You can find this information on our website. If you need additional resources, please contact us.
Where can I find information about the research behind PEARLS?
You can find information about the research studies behind PEARLS, including research specific to isolation and depression, on our website. If you need additional resources or information, please feel free to contact us.
Providing PEARLS in Your Community
These are questions people often have about what to expect when providing PEARLS or questions they have about providing the program.
What is a typical PEARLS caseload?
The average PEARLS caseload depends on how much full time equivalent (FTE) you have for PEARLS coaches and whether your coaches have other duties and responsibilities, such as providing case management services or other therapies.
Ballpark Caseload Estimate
- 15-20 participants for a half-time PEARLS coach
- 30-40 participants for a full-time PEARLS coach
Some PEARLS participants are seen for weekly sessions, while others have monthly sessions and/or follow-up calls, which allows coaches to have a bigger caseload. Other factors to consider include travel time (distance and traffic) needed to get to and from appointments with PEARLS participants.
Caseload sizes also vary between organizations. Some organizations span a large geographic area, which increases the travel time to see PEARLS participants. Not all the PEARLS coaches who have dispersed clients are able carry full caseloads. Some organizations have full time coaches who carry 25-to-50-person caseloads. However, another organization may have a few part-time coaches who work a total of 30 hours per week with an average of 10-12 active cases.
A tip for maintaining your caseload is to build ample time for outreach, recruitment, screening, data entry, and supervision.
Funding source may dictate caseload size as well. Some grants or levy-funded programs aim to enroll a certain number of participants per month, quarter, or year.
How can my organization screen older adults for depression?
Some organizations currently screen for depression as part of their annual assessment or intake. If you do not already do this, you can add a brief, validated depression screening instrument (such as the PHQ-9) to your practices, which will be key to identifying older adults who may be eligible for PEARLS.
How can my organization measure individual progress or outcomes?
The University of Washington Health Promotion Research Center provides questionnaires to measure progress or outcomes for individual PEARLS participants. We will go over the questionnaires during training and provide the needed materials in the PEARLS Implementation Toolkit.
- Baseline & Final PEARLS Questionnaire: This questionnaire includes measures for self-rated health, physical activity, social activity, and pleasant activities. They help establish where the participant is when they begin the program and where they are at the end.
- Session Questionnaires: For each of the PEARLS session you will use what is known as the Patient Healthcare Questionnaire (PHQ-9). It is a brief, validated measure of depression severity used in primary care. It consists of nine questions that measure how much someone’s symptoms of depression (e.g., low energy, lack of appetite, depressed mood) are affecting them. Administering the PHQ-9 at each PEARLS session provides a way to monitor a participant’s progress throughout the program, as well as educate them about their depression symptoms.
Depression Outcomes Include:- Remission (no longer meets criteria for clinically significant depressive symptoms)
- Response ( ≥ 50% drop between baseline and final PHQ-9 score)
- Significant Change (≥ 5-point drop between baseline and final total PHQ-9 score)
These individual outcomes can be looked at collectively on a regular basis to show your organization’s impact, including the quarterly change in PHQ-9 scores for all PEARLS participants and/or the percent of participants that met remission each year.
- Participant Satisfaction Questionnaire: This allows you to see how participants felt about PEARLS, gather quotes and reactions, and evaluate where there are areas for improvement. In addition to this questionnaire, we encourage agencies to gather testimonials from participants to use for program evaluation and marketing.
How can my organization evaluate the overall program success?
In addition to individual outcomes, it is important to assess how well PEARLS is being implemented overall. This includes looking at the percentages of people that move through the program, such as referrals, people who enroll, people who complete the program, and people who enrolled but did not complete the program. You will also want to look at whether key program components are in place, such as regular clinical supervision meetings.
The PEARLS Implementation Toolkit offers one model for evaluating program implementation, including examining program reach, effectiveness, adoption, implementation, and maintenance.
Sticking to the PEARLS Protocol & Model
We have developed a tool to help organizations assess whether they are staying within the PEARLS protocol and model (referred to as program fidelity). PEARLS coaches or program supervisors can use this brief instrument. We published a research article about the development and testing of the fidelity instrument. A link to the instrument we tested can be found along the right-hand side of the research article webpage (Click “Open Supplemental Data”).
The PEARLS Implementation Toolkit also includes a coach self-assessment as well as a checklist to help coaches remember key components of sessions.
Please contact us with any questions about fidelity and balancing fidelity with program adaptations.
How can my organization collect and track data for PEARLS?
Regular data collection is important for monitoring individual PEARLS success and adjusting as needed. Tracking data also allows an organization to monitor and evaluate the program’s benefits and challenges. The PEARLS Implementation Toolkit provides forms needed for data collection as well as several spreadsheets to facilitate data management.
Data Tracking Options
- WellWare: We teamed up with Sound Generations to create this online data management system. Its features include tracking referrals and participants, process and outcome reports, and downloadable forms in Word and PDF format. The system is built on Salesforce’s secure cloud platform that is widely used in healthcare, financial industries, and government agencies.
- Cost: $200 per year per single user license
- Contact: Meghan Thompson, Sound Generation
meghant@soundgenerations.org
206-268-6701
- PEARLS Provided Resources: We provide a survey data excel sheet in the PEARLS Implementation Toolkit.
- Develop Your Own Excel Sheet or Use Your Existing Data Systems: Some organizations have developed their own excel sheet(s) to track PEARLS data, while others use their existing data systems, such as ReferNET or PeerPlace databases.
Are there tips for administering the PHQ-9 (the nine questions done during PEARLS sessions)?
We recommend having the PEARLS coach read the nine questions in the PHQ-9 as stated on the form to ensure you are sticking to the PEARLS protocol and model (referred to as program fidelity).
The name PHQ-9 may not mean anything to PEARLS participants. Some PEARLS coaches refer to the PHQ-9 as the nine questions that they ask at the beginning of each PEARLS session to see how the participant is doing since they last met. As participants get more comfortable doing the PHQ-9 and talking about depression, the questions become a tool for teaching them about their symptoms of depression and how to monitor them (like with monitoring their blood pressure or sugar for people living with hypertension and diabetes).
Yes/No Framing & Using a Scale
It may be easiest to phrase PHQ-9 questions as a Yes/No and use visuals to help PEARLS participants answer, such as this visual scale or a calendar to display the past two weeks.
Timing
We recommend that coaches administer the PHQ-9 at the beginning of the session. However, participants may have a strong desire to talk about particular topics or events, so it is okay to cath up a bit and then administer the PHQ-9.
Additional Resources
More tips about administering the PHQ-9 can be found in the PEARLS Implementation Toolkit’s section on PEARLS sessions.
The Mental Health Training Network also offers a free, self-paced online training on the PHQ-9 that is geared towards working with older adults.
What if a participant’s PHQ-9 results become stagnant?
Consult your clinical supervisor about how the PEARLS participant is doing with their Problem-Solving Treatment and Behavioral Activation if a participant’s PHQ-9 score becomes stagnant. Work with the clinical supervisor to examine other things that could be affecting the participant’s depression.
Score Fluctuation
PHQ-9 scores may fluctuate both ways — e.g., some participants may start with a very high score and drop significantly after the first session, while others may increase after the first session. In some cases, the fluctuation in scores may be affected by how comfortable the participant is with answering the questions, whether they believe their score is tied their ability to continue to receive services, their increased awareness about depression, and/or how long it takes them to perceive a benefit from someone visiting their home.
It may be that the participant is working on problems and activities that are not central issues to their depression. Try to explore deeper problems that they may want to address.
At times the total PHQ-9 score stays the same but there may be improvements in some of the questions and decreases in other questions. A participant’s score could also stay the same even if they have made positive changes in their lives. Remember to point out the participant’s successes, even if they are small.
Can we repeat or pause PEARLS sessions?
Setbacks can create scheduling issues or disrupt the frequency of sessions. When a trauma happens in the middle of PEARLS sessions, work with your clinical supervisor to possibly meet the participant more frequently to get on top of the new problem or setback.
It is okay to pause PEARLS sessions for one to two months if a participant is away or in the hospital. When resuming sessions, you may need to meet more frequently at first to get the participant back on track. You are still aiming for a total of eight session.
After a setback, resume weekly sessions initially to reinforce skills even if the participant is further along in the program.
If a caseload permits, it is okay to repeat PEARLS a second time. If the participant is requesting to go through the program a third time, there may be other underlying issues that need to be addressed outside of PEARLS, including that some participants enjoy having a visitor. Many communities offer free services for friendly visits.
Do PEARLS coaches have to do both Problem-Solving Treatment and Behavioral Activation during each PEARLS session?
While we encourage and teach Problem-Solving Treatment and Behavioral Activation (social, physical, and pleasant events scheduling) at each PEARLS session, it is okay if only one happens during a PEARLS session given other circumstances.
Some participants are resistant to doing Problem-Solving Treatment because this type of approach is not something that they are familiar with or does not resonate with their worldview. One way to address this is to teach problem-solving skills using barriers that come up when doing Behavioral Activation. For example, if the participant is unable to walk around their neighborhood because of safety concerns, the PEARLS coach and participant can work through seven problem-solving steps to identify other ways to be physically active such as walking during the day with a neighbor or doing seated exercises in their living room.
Other participants might prefer to just work on only Problem-Solving Treatment, skipping a physical activity for that week, for reasons such as feeling ill.
Can my organization provide other therapies during PEARLS sessions?
The original PEARLS research focused on two evidence-based treatments — Problem-Solving Treatment (PST) and Behavioral Activation (BA). We encourage PEARLS coaches to stay focused on delivering those two treatments during PEARLS sessions to teach older adults skills to manage their depression.
Why just those two?
If you do other treatments during PEARLS sessions, you can never be sure that you are giving someone an adequate dose of any psychotherapy, and the evidence-base requires a certain amount of Problem-Solving Treatment and Behavioral Activation.
When are other psychotherapies okay?
It is okay to do other psychotherapies:
- After the PEARLS sessions have ended; OR
- While PEARLS is in progress if the other psychotherapies are with a separate staff member or PEARLS coach AND not during the same time as the PEARLS session.
How do I handle inappropriate behavior or issues from a participant?
If a participant is being inappropriate toward a PEARLS coach, have the coach set firm boundaries around the type of language or behavior that is not okay. It may be appropriate for other staff to accompany the coach on initial visits if they are uncomfortable.
Look into participant history and assess potential safety and other issues. Participants may need to be referred to other therapy resources such as mental health or addiction services.
Some older adults may have bedbug or insect issues. Coaches should bring minimal things such as their own chair and disinfect their items with alcohol after the sessions (not in front of the participant). You could also try to meet in a community setting that is convenient for the participant and private.
Spreading the Word About PEARLS
These are questions people have about promoting or sharing PEARLS information with their community and potential PEARLS participants. Organizations should feel free to rename the program, use a different word for PEARLS coaches, and/or brand the program as they see fit for their community’s needs.
Are there suggestions on how to recruit PEARLS participants?
PEARLS participants can come from referrals within your organization or from outside your organization. Your organization will need to create an internal pipeline for current or inquiring clients, as well as potentially cultivating community relationships for outside referrals.
Many times, the PEARLS coach is the person doing the recruitment, although this can vary from organization to organization.
Whoever is in charge of recruitment should be prepared with materials about PEARLS. We recommend the PEARLS coach send a possible participant an introductory letter once they are referred to the program. We discuss more about marketing materials in the other questions in this section.
General Recruitment Tips
Things to keep in mind with your recruitment activities.
- Build in Recruitment Time
You’ll need time to create and nurture relationships around the community. Some organizations will have their PEARLS coach hold monthly meetings with local agencies to talk about the program and referrals. - Communicate Eligibility & Consider Your Capacity
It is important to communicate eligibility criteria for PEARLS and have sufficient capacity for processing referrals and enrolling new participants to ensure that referrals are appropriate and you do not discourage future referrals from your contacts. - Make sure referral partners know that older adults do not have to have a clinical diagnosis of depression to participate.
- Multiple Types & Points of Contact With Potential Participants
When contacting a potential PEARLS participant, it may take mailing information three times, making multiple phone calls, and/or visiting a them in-person to help them engage.
Finding Referrals
Building relationships with community-based organizations and other agencies that serve older adults and isolated populations is key to successful recruitment outside your organization. Begin networking by attending local health and aging events in your community. Connect with people from the following organizations:
- Senior Centers
- Religious Institutions
- Clinics
- Assisted Living Facilities
- Senior Housing
- Meal Delivery Programs: Meals on Wheels, etc.
- Media Sources: newspapers, TV, and radio
- Housing Authorities
- Adult Protective Agencies
- Veterans Health Administration (VA)
- Rehabilitative Units
- Addiction Treatment and Support Programs
- Emergency Responders: firefighters, 911, and/or emergency medical technicians (EMTs)
- Healthcare Providers: neurologists, primary care physicians, geriatric physicians, nurses, social workers
- Transportation Assistance Programs and Services
- Hair Stylists
- PEARLS Participants (they can refer friends and family based on their experience)
Promotional & Relationship Building Activities
Putting on events can bring awareness to the issue of depression and isolation for older adults and PEARLS as a solution.
- Hold a presentation for agencies and community partners about depression, aging, isolation, and PEARLS. Provide food (if possible).
- Hold a presentation for potential participants on wellness education, feeling better, and/or becoming more self-sufficient or social where they could enter to win a gift if they complete a two-question survey (the PHQ-2) and provide their contact information.
- Hold a training on how to screen for depression (using the PHQ-2 or PHQ-9) and make referrals to your organization for PEARLS.
- Consider topical or timely promotion times, such as May. It is both Mental Health Month and Older Adults Month.
Connecting With a Possible PEARLS Participant
When you do contact and connect with a potential PEARLS participant for the first time, it is important to be delicate in the way you discuss and describe the program. About 75% of PEARLS participants do not know that they are depressed or experiencing mental health issues. Approach the initial call as if they do not know. It’s more important for them to get their foot in the door instead of convincing them that they are depressed.
After you have a referral, contact the potential participant on the phone or in-person as soon as possible (24-48 hours). Calls may take 5-20 minutes. Initial one-on-one contact could include discussing:
- The program focuses on developing skills and problem-solving to address issues that may be making them feel unpleasant or sad so they can improve their health, happiness, and quality of life.
- PEARLS takes place in their home or a community setting that works for them.
- The program is for older adults who might be experiencing multiple health issues, have difficult family dynamics, or want to be more self-sufficient.
- It’s a collaborative effort with a coach, and they will decide which issues in their life they want to tackle. They are in the driver’s seat.
- They will work with the PEARLS coach on establishing goals they want to achieve and collaboratively brainstorm ways to achieve those goals.
- While there is a fair amount of paperwork during the first PEARLS session, the coach will help them complete it.
Some organizations encourage the referral source to be present at the first three sessions to help build rapport and trust between the coach and participant if the participant is from a community that has had negative experiences with services or health systems.
Are there tips for recruiting underserved populations?
Here are a few suggestions on how you can improve your recruiting efforts with underserved communities.
- Consider renaming PEARLS to something that better suits your organization or the community you are trying to reach.
- Connect with community representatives to learn how to best reach potential participants. This could include representatives from religious centers, veteran organizations, cultural centers, and/or neighborhood resources, etc.
- It is okay to use forms that have been translated and reviewed by members of the community. If you translate forms, please share them with us so we can make them available to other organizations as needed.
- Be aware that some cultures may be apprehensive about paperwork and signing documents if they have had negative historical experiences (this could include immigrants and/or Native American communities).
- Consider using words that will make sense to the greatest number of people in a community. Also think about how to best reach and connect with people who have limited-English skills.
- Make sure materials are appropriate in terms of literacy, culture, images, and spiritual backgrounds.
Are there samples or templates for PEARLS flyers or brochures?
Yes, we have sample and template materials for organizations to use. They can be found here on our Google Drive. Please feel free to adapt the branding to meet your organization and community needs. You can even rename PEARLS.
Are there tips for creating informational materials about PEARLS?
Yes, we have some tips and ideas for your PEARLS materials.
Avoid Stigmatizing Words
You might want to avoid using the terms like depression, mental health, or counseling (or other terms you know would not resonant well with your community). You can use terms and phrases like wellness, well-being, mood, emotion, feel better, quality of life, problem-solve, skills for more independence, etc. Use terms and phrases that will resonate with the communities you are trying to reach.
Success Stories
Include success stories in your PEARLS materials. You can use stories from our website to help get you started.